

Tomorrow, President Biden will deliver a State of the Union Address to a joint session of Congress. Most of this newsletter examines the health policy issues that the president may bring up. But first I recap a presentation I gave last week at the American Enterprise Institute, which C-SPAN covered live, and I highlight a virtual discussion that Paragon is hosting tomorrow on Medicare Advantage.
Correcting the Record on the ACA
On March 1, AEI hosted an event on the Affordable Care Act. Here is a video of my remarks, and the text. Here are a few of the key points I made:
- The ACA in 2024 is largely the law that the health care industry would have written. It just took some time to get to it. The main components that the industry liked—large new subsidies through Medicaid expansion, the exchanges, and 340B—are growing. The main components that the industry disliked, including most of the taxes, have disappeared.
- The ACA has significantly increased deficits and central elements that were meant to drive health care savings like the Centers for Medicare and Medicaid Innovation have failed.
- The 2017 legislative efforts were centered on reforming or modifying the ACA and were not about repealing and replacing the law.
- The Trump administration did not engage in sabotage of the ACA, as is often alleged. To comply with a federal court ruling forbidding certain payments to plans without a Congressional appropriation, regulators permitted silver-loading, which boosted ACA subsidies. The administration also allowed individual coverage health reimbursement arrangements, which increase ACA individual market enrollment using employer contributions.
With respect to key ACA problems, I suggested two major reforms:
- End the federal discrimination against lower-income children and people with disabilities on Medicaid by reducing the much higher federal reimbursement rates for the ACA Medicaid expansion population of non-disabled, working-age adults to the federal rate states receive for the other populations.
- Create a better targeted, more efficient subsidy structure and end the enhanced subsidies which benefit insurers and inflate total health care spending.
Paragon Event on Medicare Advantage Tomorrow
Tomorrow, March 7, at 1pm EST, Paragon will host a virtual discussion of MA and Paragon’s new paper, Improving Medicare Through Medicare Advantage. The discussion will feature Paragon’s Demetrios Kouzoukas and Joe Albanese, Loren Adler of the Brookings Institution, Josh Gordon of the Committee for a Responsible Federal Budget, and Chris Pope of the Manhattan Institute. Register for the event here.
The State of Health Policy
The president will likely raise several health policy items tomorrow during the State of the Union. In anticipation, Paragon wants to make sure that the ensuing discussion contains full perspective.
ACA Enrollment and Subsidies
President Biden signed legislation that significantly increased subsidies to health insurers for people who purchase ACA exchange plans. These enhanced subsidies are deeply problematic, raising wasteful spending and giving health insurers enormous power to increase premiums with the full cost borne by taxpayers.
These subsidies have significantly increased enrollment in the exchanges, particularly among lower-income enrollees who now pay nothing for coverage. While President Biden may tout record enrollment, it is important to acknowledge that the enrollment is driven by tens of billions of additional subsidies to health insurers and that most enrollees now signing up with free plans did not find enough value in the plans when the cost was only about $25 a month to them to enroll.
Drug Pricing
President Biden will likely raise Medicare’s new price controls on prescription drugs mandated by the Inflation Reduction Act. He will likely not mention that price competition had already constrained Medicare Part D annual per beneficiary spending growth to 2.6 percent over the past decade.
The president may tout his “cancer moonshot” which he claims will “end cancer as we know it.” Yet, his policies will lead to fewer innovative, life-saving therapies coming to market. The burden will likely fall disproportionately on cancer drug development as at least half of new drugs in the pipeline are oncology drugs. The costs of developing cancer drugs are higher than other therapeutic areas, and companies will be less likely to develop cancer drugs when the potential return is artificially constrained.
The $35 cap on insulin in Medicare will be another applause line that is separated from reality. Before this policy was put in place, insulin copays were already decreasing due to new biosimilar competition — over 75 percent of insured insulin users already had copays under $35. Ironically, copay caps are favored by the largest incumbent insulin manufacturers because they mitigate price competition from cheaper alternatives.
Medicaid Expansion
President Biden may refer to Medicaid expansion and bemoan states that have yet to adopt expansion. A recent Paragon report, which focused on Florida, shows that states that have refused to adopt the ACA’s massive expansion of the program have made the right call for several reasons:
- Medicaid expansion does not improve population health.
- Expansion produces a surge of spending for able-bodied, working-age adults but reduces health care access for traditional Medicaid enrollees.
- After expansion, Medicaid enrollees were one-third less likely to obtain doctor appointments, leading to a surge of emergency room visits for non-emergent care.
- Expansion significantly decreases the number of workers per Medicaid recipient.
- Expansion leads to much higher federal deficits.
- Expansion produces a surge of improper payments and wasteful spending.
- Expansion makes states further dependent on the federal government for financing.
Medicare Financing
At last year’s State of the Union, President Biden declared “if anyone tries to cut Medicare, we’re going to stop it.” A spirited back-and-forth with members of both parties seemed to confirm that such policies were off the table.
But, as today’s Paragon Pic below shows, legislation signed by Biden as president and when he was vice-president significantly reduced projected Medicare spending.
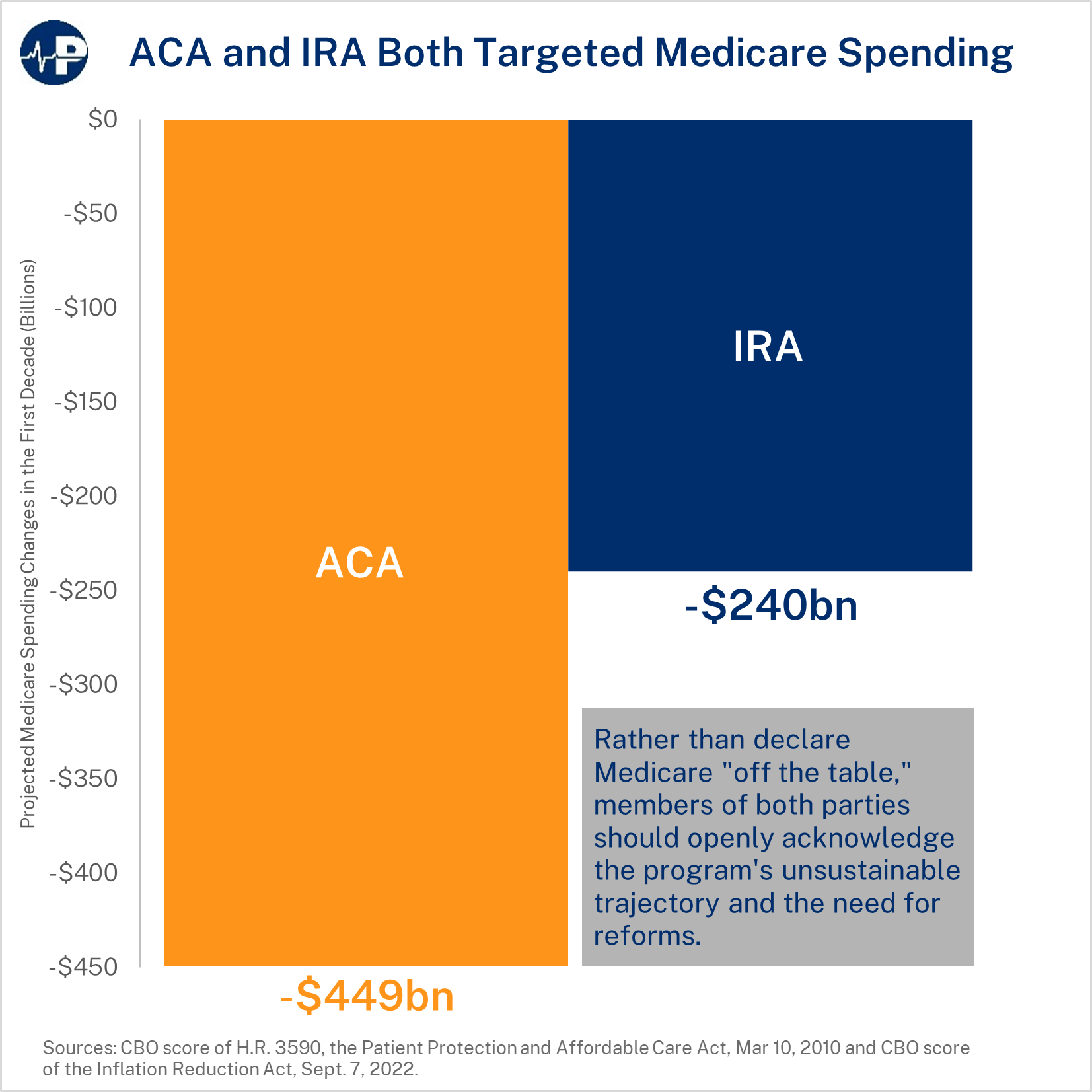
Medicare faces enormous financial challenges, both with the pending insolvency of the Hospital Insurance (Part A) trust fund as well as with massive future unfunded liabilities. Policymakers should pursue policies that create a more efficient Medicare program; however, they should not use Medicare as a piggybank—as both the ACA and the Inflation Reduction Act did—to expand other government programs.
See here for the full analysis around this week’s Paragon Pic.
All the best,
Brian Blase
President
Paragon Health Institute
