
Brian Blase, Ph.D.
Brian Blase, Ph.D., is the President of Paragon Health Institute. Brian was Special Assistant to the President for Economic Policy…
Reforming Government. Empowering Patients.
Navigation
This paper reviews the effects and risks that Medicaid expansion would have on the state of Florida.
Federal dollars have enticed 40 states plus the District of Columbia to expand the Medicaid welfare program to able-bodied, working-age adults under the provisions of the Affordable Care Act (ACA). While expansion does deliver additional federal funding to states and lead uninsured and previously privately insured residents to enroll in the program, there are significant drawbacks to expansion.
The actuarial consulting firm Milliman estimates that expansion in Florida would lead to 2.13 million additional Medicaid enrollees by 2029 with a projected cost of $123 billion over the 2025-2034 period. Under a high estimate, which accounts for higher enrollment and uses cost growth projections from the Congressional Budget Office, expansion enrollment would be 2.63 million with a projected cost of $176 billion. Although federal taxpayers would bear most of these costs, the respective costs to Florida would be between $11.1 billion and $17.2 billion under these scenarios.
Milliman estimates that Medicaid enrollment would increase between 47.4 percent and 59.8 percent, and Medicaid spending would increase by between 30.4 percent and 42.8 percent if Florida expands Medicaid. States that have expanded their Medicaid programs typically have much higher enrollment and spending than projected. If Florida adopts the ACA’s Medicaid expansion, approximately 30 percent of Floridians would be enrolled in the program, and there would only be 1.5 workers for every Medicaid recipient.
Overall enrollment exceeded projections by more than 50 percent on average in states that expanded Medicaid under the ACA, and spending exceeded projections by a third. Importantly, if the trends from other states continue in Florida, the state could expect total expansion enrollment of more than 3 million people with state costs between $15 billion and $26 billion over the 2025-2034 period.
Florida’s favorable tax and spending climate, with no state income tax and per capita spending far below the national average, has contributed to both population and economic growth in the state. If Florida expands Medicaid, the state would need to raise much more revenue, and Medicaid would further crowd out other state priorities such as education, infrastructure, and transportation. If Florida expands Medicaid, Medicaid spending as a share of the state budget, inclusive of federal dollars, would increase from 31 percent to about 40 percent or more using Milliman’s estimates.
As states expanded Medicaid, the national Medicaid improper payment rate nearly quadrupled. If these trends hold for Florida, improper payments in Florida’s Medicaid program would rise by billions of dollars each year. Pharmaceutical fraud and abuse has been one particular area of concern with the growth of Medicaid.
Medicaid expansion would have harmful health care effects in addition to the deleterious fiscal effects. Expansion would lead to greater health care access challenges for existing enrollees. Recent research demonstrates that expansion has resulted in states shifting resources from traditional Medicaid enrollees, such as children and people with disabilities, and toward able-bodied, working-aged adults while creating a disincentive to work.
Under expansion, Medicaid recipients have more difficulty obtaining primary care appointments, experience longer wait times for specialty care, and wait longer for ambulances. According to Milliman’s projections, 65 percent of the people who would gain Medicaid in Florida would replace private coverage, which offers better access to both primary and specialty care appointments. Because Medicaid enrollees struggle obtaining appointments, Medicaid expansion results in a significant increase in emergency department utilization. Based on the experience of other states, if Florida expands Medicaid, it would be more challenging for existing Medicaid recipients to obtain appointments.
The health effects of Medicaid expansion have been disappointing, and expansion may in fact lead to worse overall population health. Several studies—including the Oregon Medicaid experiment, which randomly assigned people into Medicaid—find that Medicaid enrollment does not improve physical health outcomes. Expansion could lead to worse overall health outcomes if it reallocates services away from people who need them more to people who benefit less from the additional services. In fact, from 2013 through 2017 (the first four years of the ACA’s Medicaid expansion), the mortality rate worsened in expansion states relative to non-expansion states, as Medicaid expansion states had worse opioid-related mortality.
Although hospitals lobby for Medicaid expansion, it is not clear that they benefit from it. Part of this is because people replace private coverage that pays higher rates with public coverage that pays lower rates. Regardless, Florida’s hospitals are extremely profitable now, with profit margins well above the national average, and they certainly do not need additional revenue from taxpayers or to become further dependent on government programs for their revenue. The expansion’s main economic effect seems to be producing a windfall for health insurers at taxpayers’ expense.
Florida’s costs could increase much more depending on future policy changes. If Florida adopts Medicaid expansion and the enhanced federal medical assistance percentage (FMAP) is lowered to the normal FMAP, the state would be on the hook for an additional $40.5 billion from 2025 to 2033. And this outcome is a real possibility. Lawmakers in Florida, particularly those who consider themselves fiscal conservatives, should be skeptical of expansion because of the precarious federal fiscal position. Within the next decade, Congress will be forced to deal with the significant fiscal pressures that government entitlement programs are placing on the federal budget. When this happens, lowering the FMAP for the expansion population—which President Obama proposed in his 2012 budget and which passed the House of Representatives in 2017—will be under consideration.
The conclusion is clear: Florida has made the right decision to not expand Medicaid under the ACA thus far. Expanding would necessitate higher state taxes, force cuts to other state priorities, and reduce access to care for traditional Medicaid enrollees and many new Medicaid enrollees, most of whom would replace private coverage with Medicaid. Expansion would lead to a surge of improper payments and unnecessary emergency department use. There is no evidence that Floridians overall would receive health benefits from expansion, and the financial impact on hospitals is unclear. Adopting Medicaid expansion would make Florida increasingly dependent on the federal government and vulnerable when the federal government eventually lowers the enhanced rate for the expansion population.
Medicaid was created in 1965 as a joint federal-state public welfare program to finance medical services and long-term care expenses for certain categories of low-income people. Although state participation in Medicaid is optional, all states have participated since 1982. The federal government sets broad rules for the program around eligibility and benefits and provides an open-ended reimbursement of state Medicaid expenditures, referred to as the federal medical assistance percentage (FMAP).
For traditional Medicaid enrollment categories—low-income children, pregnant women, seniors, and people with disabilities—the FMAP is largely a function of state per capita income.1 Poorer states have a higher FMAP, and richer states have a lower FMAP. The federal government sets an FMAP floor of 50 percent in the wealthiest states. The FMAP structure was intended to provide additional federal support in poorer states, as richer states have greater fiscal capacity to finance Medicaid. However, richer states receive more federal money both per capita and per person in poverty to support their Medicaid programs, because they typically have much more expansive and expensive programs.
The Affordable Care Act (ACA) contained a significant Medicaid expansion to able-bodied, working-age adults in households below 138 percent of the federal poverty level (FPL)— $20,120 for a single person and $41,400 for a household of four in 2023. Prior to the ACA, a few states permitted at least some low-income, working-age, childless adults to enroll in Medicaid.2
In a 2012 ruling, the U.S. Supreme Court made the expansion optional for states. When the expansion took effect in 2014, 23 states plus the District of Columbia had adopted it.3 Currently, 40 states plus the District have adopted the ACA’s Medicaid expansion. Interest groups—principally health insurers and hospitals put enormous pressure on state lawmakers to adopt expansion.
To incentivize states to expand Medicaid, the ACA set the FMAP for the expansion population at a much higher rate: 100 percent from 2014 to 2016 and then gradually declining to 90 percent in 2020, where it is scheduled to remain. There are several consequences from a much higher FMAP for the ACA expansion population than for traditional Medicaid enrollees. First, the differential means that the federal government discriminates against the traditional—and generally much needier—Medicaid populations in favor of the able-bodied, working-age adult population. Second, as demonstrated by new research, expansion states are taking resources away from traditional populations and reallocating them to expansion enrollees with some evidence of worse outcomes for traditional enrollees.4 Third, a higher FMAP for the expansion population has led to substantially higher spending in the program, including much higher improper payments. Roughly one in four dollars expended through Medicaid nationally does not meet program rules, up from a 6 percent improper payment rate before the expansion took effect.5
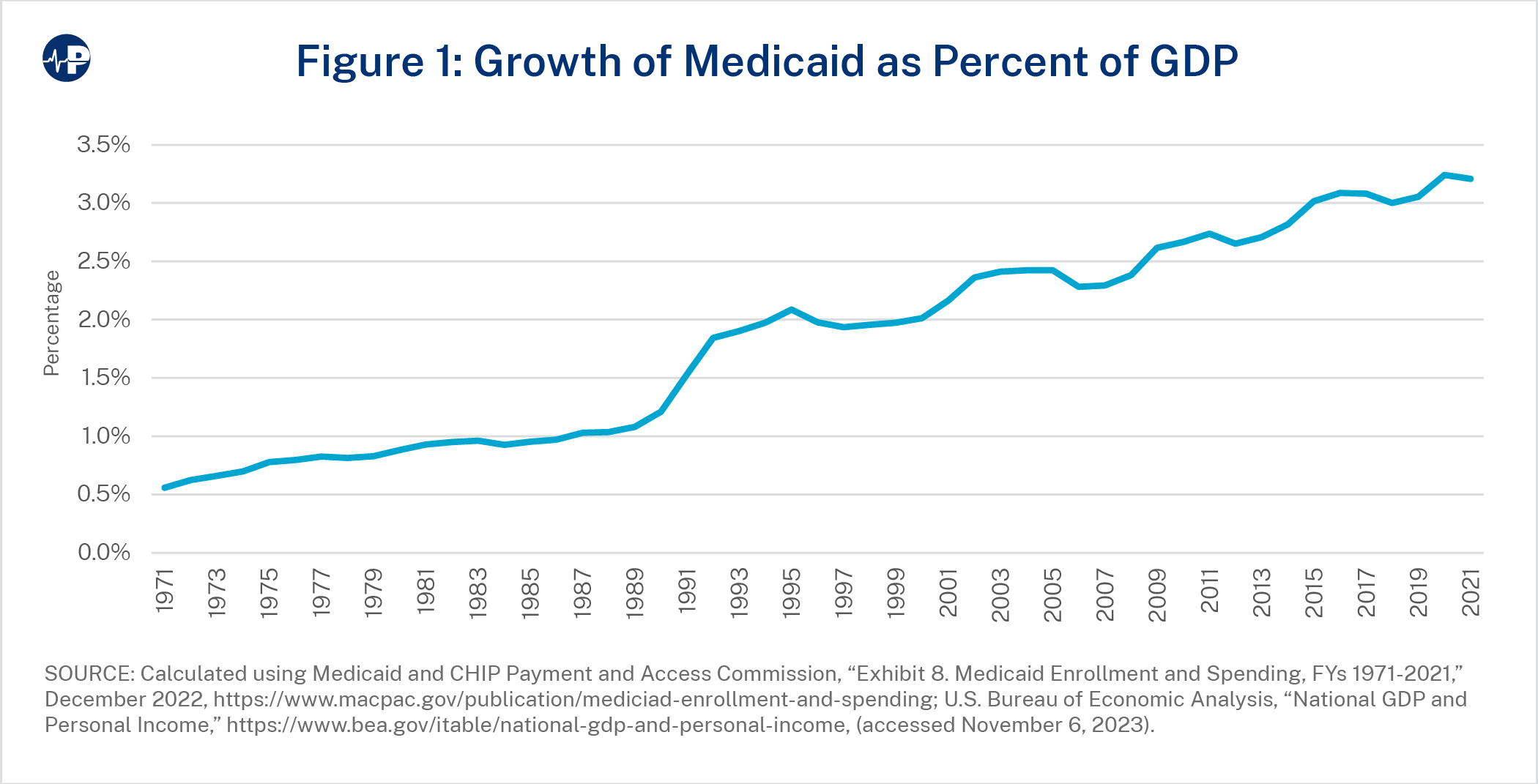
The best way to understand Medicaid’s economic cost is the percentage of gross domestic product (GDP) expended through the program. In 1970, Medicaid represented 0.5 percent of U.S. GDP; in 1980, 0.9 percent; in 1990, 1.2 percent; in 2000, 2 percent, in 2010, 2.7 percent, and in 2020, 3.2 percent.6 This indicates Medicaid has consistently grown faster than the overall economy has. Figure 1 shows the growth of Medicaid’s total cost as a percentage of U.S. economic output over time.
Starting in April 2020, enrollment in Medicaid began to rapidly increase because of the COVID-19 pandemic and government pandemic policies. The pandemic caused some people to lose their jobs and employer-sponsored coverage and become eligible for Medicaid. The main reason for enrollment growth was a continuous coverage provision that prevented states from removing any Medicaid enrollees, regardless of whether they were eligible, for the duration of the public health emergency. By April 2023, an estimated 18 million people enrolled in Medicaid because of these continuous coverage provisions no longer met eligibility requirements for the program.7 In the spring of 2023, states began assessing eligibility and removing ineligible enrollees from the program.
Including federal dollars, Medicaid is the largest item in state budgets, eclipsing elementary and secondary education in 2003. In 2020, Medicaid accounted for 28.3 percent of total state expenditures.8 Figure 2 shows the growth of inflation-adjusted, or real, state expenditures between fiscal years 1988 and 2021. Between 1988 and 2021, real state expenditures increased by 175 percent, while Medicaid spending increased by nearly 600 percent. During that period, 35 percent of the growth in total state expenditures was driven by Medicaid.
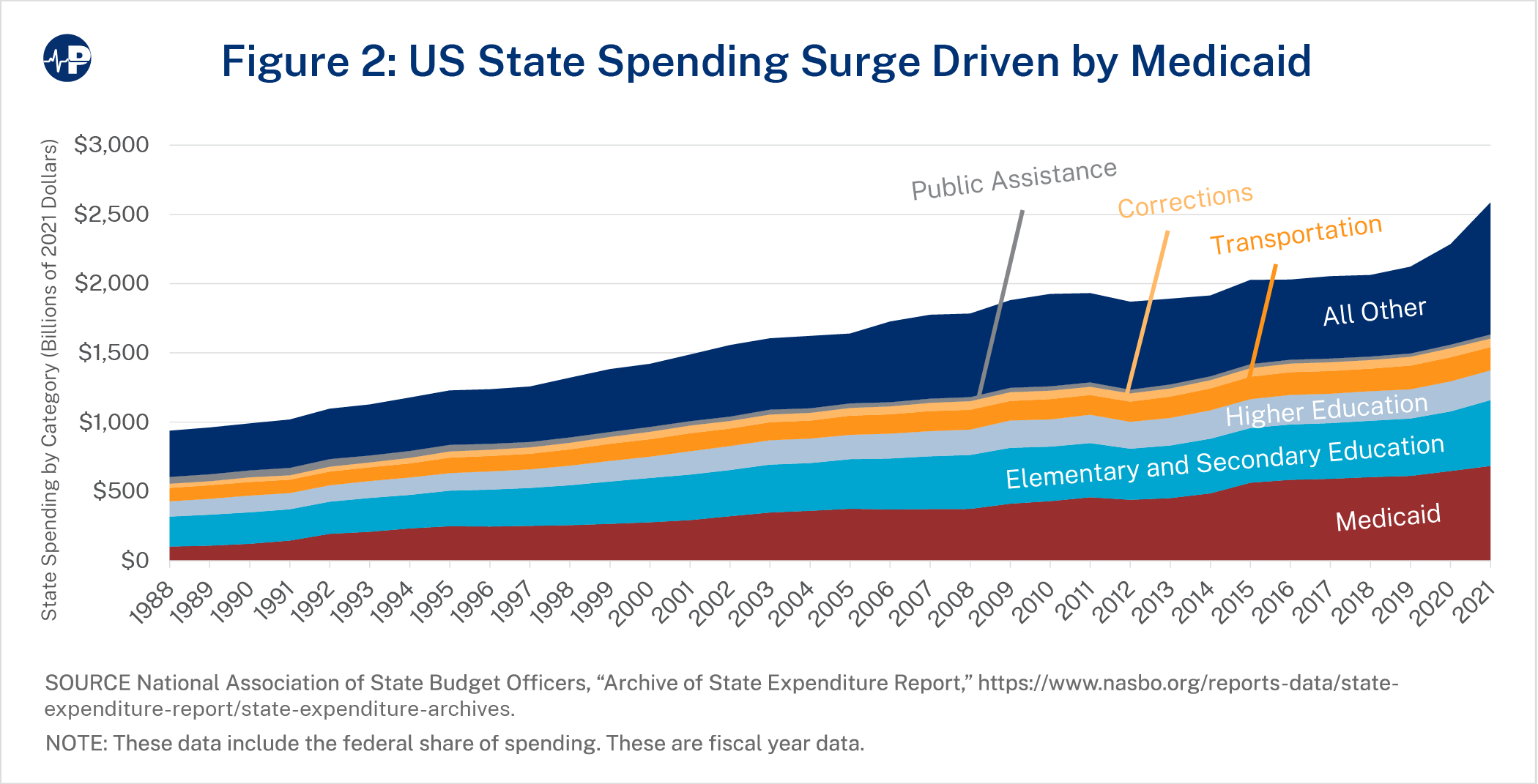
As a higher percentage of state spending has gone to Medicaid, less has gone to other major categories, such as elementary and secondary education, higher education, public safety, and infrastructure. In 1988, states spent more than three times more on education—elementary and secondary plus higher education—than on Medicaid. The National Association of State Budget Officers (NASBO) estimates that state spending on Medicaid surpassed state spending on all education in 2022.9
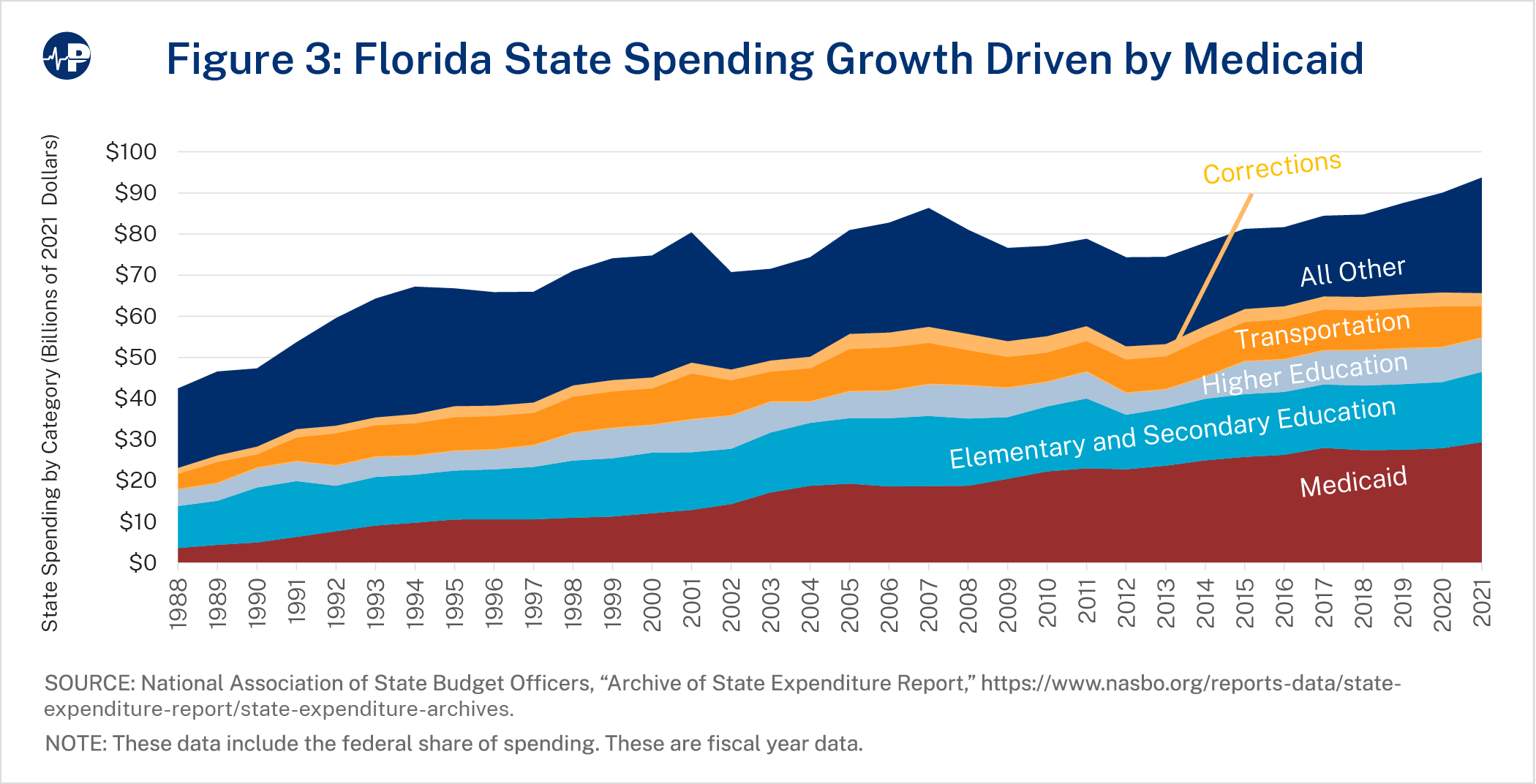
Even without expansion, Medicaid accounted for 31.0 percent of Florida expenditures in 2020.10 Figure 3 shows the growth of Florida expenditures between fiscal years 1988 and 2021, adjusting for inflation. Between 1988 and 2021, inflation-adjusted Florida government expenditures increased by 120 percent, while Medicaid spending increased by more than 700 percent. During that period, more than half the growth in state expenditures was driven by Medicaid. Thus, Medicaid’s cannibalization of the state budget has already happened to a more significant extent in Florida than in most other states. In fiscal year 2022, Florida spent approximately $38.3 billion on Medicaid, far higher than the combined spending on education $24.9 billion.11
If Florida expands Medicaid, Medicaid’s cannibalization of the state budget would be even more dramatic. Using estimates from the actuarial consulting firm Milliman, under expansion, Medicaid spending as a share of the state budget would increase from 31 percent to about 40 percent or more.12
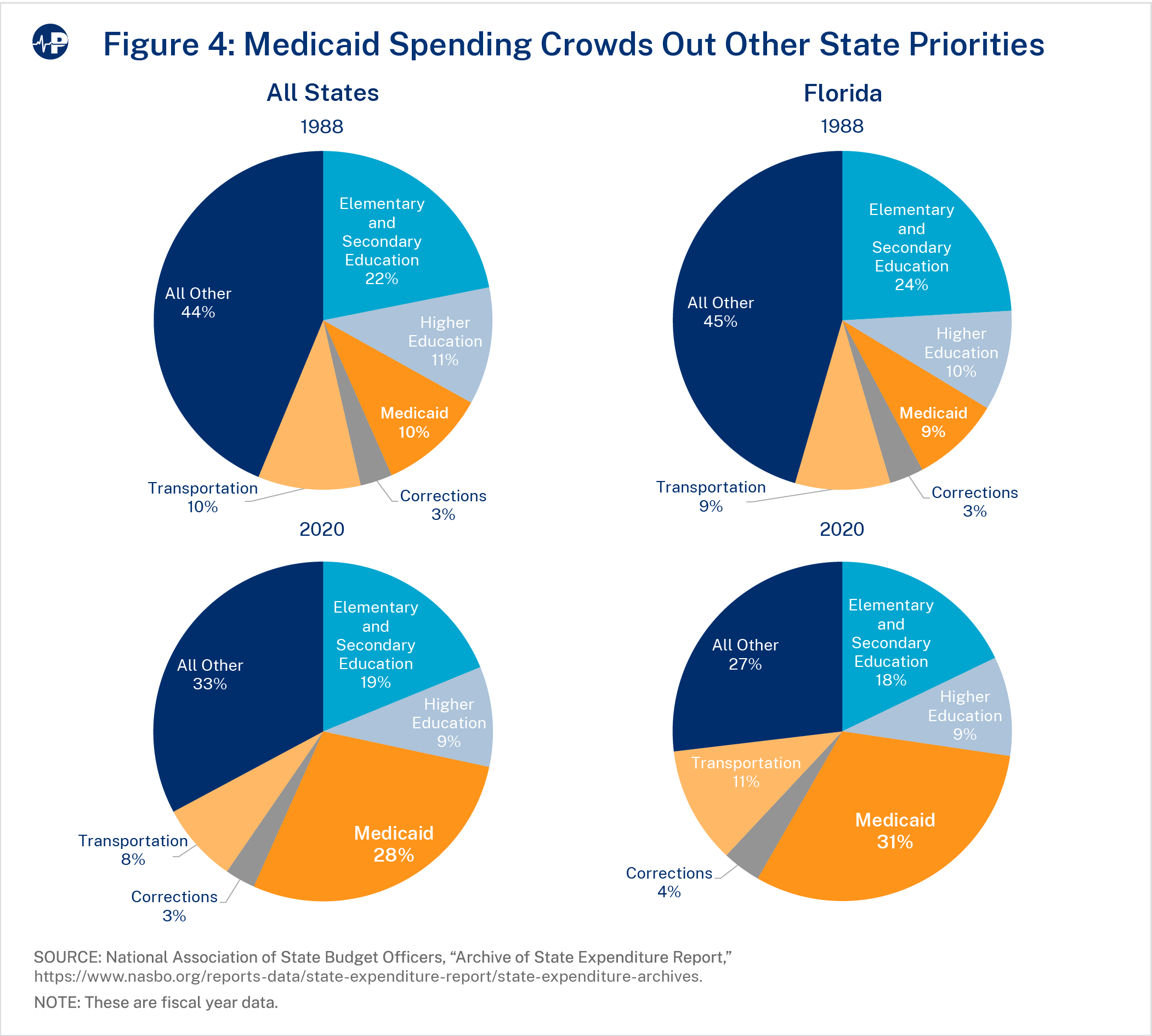
Figure 4 shows the degree that Medicaid has crowded out other areas of the state budget. The four pie charts show state spending, inclusive of federal funds, across key categories in 1988 and 2020 for all the states as well as just for Florida. Nationally, Medicaid rose from 10 percent of the average state budget to 28 percent, with less of the budget going to just about every other area. In Florida, Medicaid’s growth relative to other areas of state spending was even more dramatic, rising from 9 percent of state spending in 1988 to 31 percent of state spending in 2020. We used 2020 for the end year to avoid capturing too many of the effects of COVID-19 and the continuous coverage provisions.
Constitutionally or statutorily, most states, including Florida, must balance their budgets.13 Regardless of the federal financial enticement to expand, states still must produce a sizeable amount of revenue to finance the expansion population. Such financing would be counter to Florida’s historical position as a fiscally prudent state. Inclusive of federal grants, Florida’s per capita expenditures equaled about $4,290 in 2021—45 percent below the national average of about $7,790.14 Between 1988 and 2021, per capita state expenditures increased by about $2,790 in Florida compared to an increase of $3,950 nationally.15 The historical low-tax (Florida does not have a state income tax) and low-spend position of the state has made for an attractive fiscal climate that has helped Florida attract so many residents from around the country and contribute to strong economic growth.
According to the mid-range of estimates from Milliman, if Florida adopts Medicaid expansion, the 10-year total cost would be $123 billion, with state costs of $11.1 billion.16 However, Milliman’s mid-range estimate assumes a significantly lower growth rate in per capita costs than does the Congressional Budget Office (CBO).17 Using CBO’s expected growth rate raises the respective 10-year costs to $176 billion and $17.2 billion.18 Milliman’s high estimate also — includes higher enrollment take-up. Table 1 provides a summary of Milliman’s key estimates along with other important metrics calculated using Milliman’s estimates.19
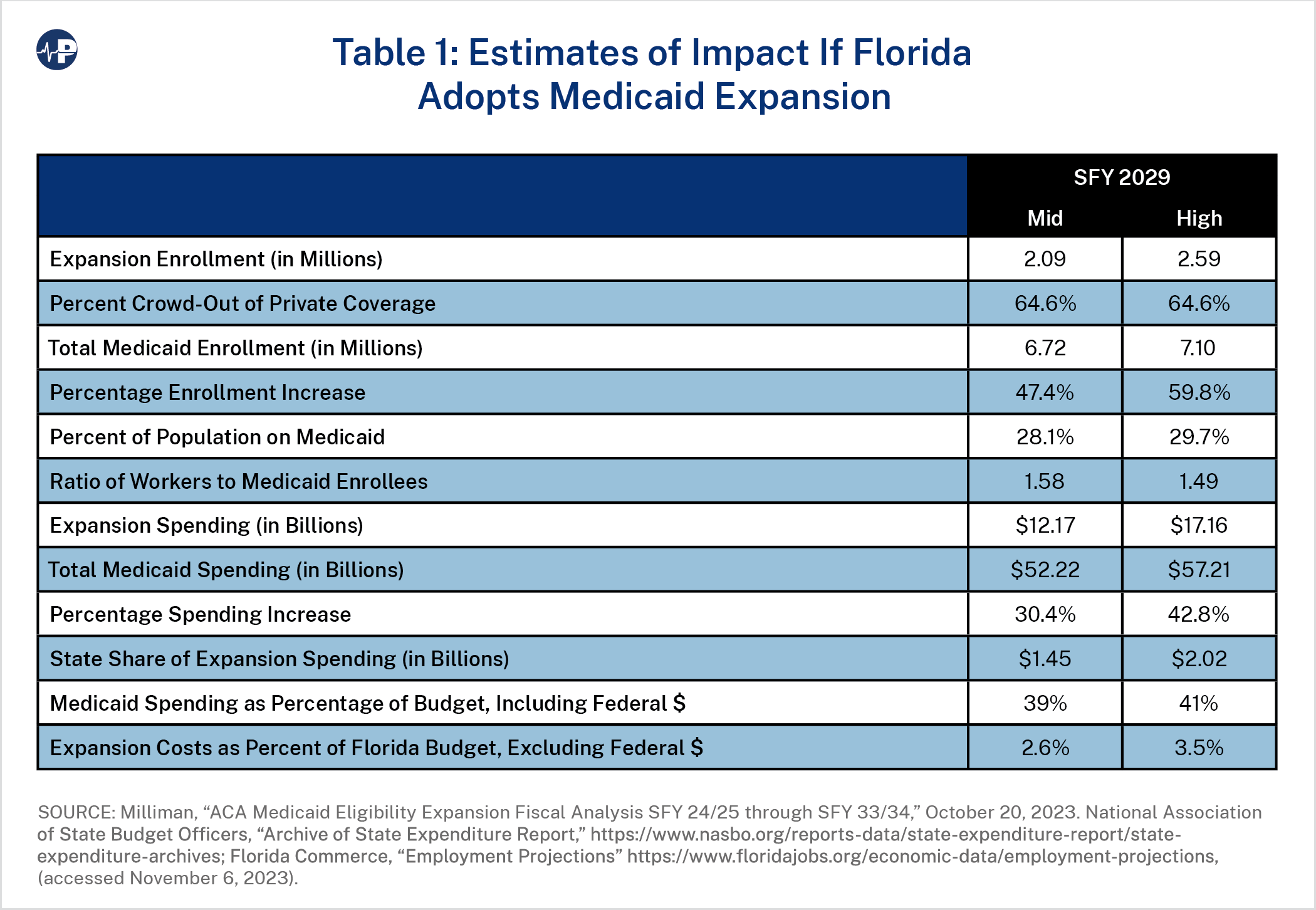
In state fiscal year 2029,20 the total cost of the expansion under the mid-range assumptions would be $12.17 billion, the total Medicaid spending would be $52.22 billion, and the state share of the expansion costs would be $1.45 billion. State costs of this amount would equal about 2.6 percent of the Florida budget, meaning that the state would need to cut about that much from other programs to afford its share of the expansion cost unless it raises taxes.21 Under Milliman’s high estimates, which use CBO’s per capita expenditures, the total expansion cost in that year is $17.16 billion, total Medicaid spending would be $57.21 billion, and the state share of the expansion costs would be $2.02 billion.22
Under the respective mid-range and high estimates, Medicaid enrollment would increase by 47.4 percent and 59.8 percent, respectively. Total Medicaid spending would increase by 30.4 percent and 42.8 percent respectively, and the Medicaid spending as a percentage of the state’s budget would increase to 39 percent or 41 percent from 31 percent in 2020.23 Expansion will likely affect Florida’s complicated Medicaid supplemental payment programs, but these effects are beyond the scope of this project.
As a measure of the potential tax burden, extra state costs of $2 billion per year translate into about 3.5 percent of the state expenditures, exclusive of federal funds.24 For example, if funded by an increase in the state’s sales tax, a $2 billion increase in state spending would need a 6.7 percent increase in the state’s sales tax, from 6.0 percent to 6.4 percent.25
The state costs largely result from the millions of people brought onto the Medicaid program by 2029, which Milliman estimates would be about 2.13 million people under the mid-range assumptions and 2.63 million people under the high-range assumptions. According to Milliman, there would be about 4.6 million Floridians enrolled in Medicaid in 2029 without expansion. Thus, under Milliman’s estimates, total Medicaid enrollment would increase to 6.72 million (mid-range estimate) and 7.10 million (high estimate). This would amount to 28.1 percent and 29.7 percent of the state population, respectively—up considerably from the 19.1 percent of the state population enrolled in Medicaid in Milliman’s non expansion baseline.
One measure of the sustainability of public welfare programs is the number of workers per welfare recipient. In February 2020—the month before the pandemic began, there were 2.51 Florida workers for each Medicaid recipient. If the state expands Medicaid, the worker to Medicaid recipient ratio will fall significantly—to 1.58 workers per recipient under the mid-range estimate and 1.49 under the high range estimate.26 About two-thirds of enrollees who gain Medicaid under expansion would replace private coverage, which, as discussed later, tends to be accepted by far more hospitals and doctors than Medicaid is.
Of the new people who enroll in Medicaid after expansion, an estimated 96.7 percent would have been made eligible by the expansion. For these people, the federal share of spending would be 90 percent.27
Milliman also projects that 71,000—or about 3.3 percent of the people newly enrolling in Medicaid by 2029—were previously eligible for the program but enrolled solely from the additional attention and outreach efforts that accompanies expansion. For these enrollees, the state would bear about 40 percent of the cost. Milliman refers to this population as the “welcome mat” population, which is also commonly referred to as the “woodwork” population. The cost of these enrollees would be approximately $2.9 billion over the 10-year projection period, with the state’s share approximately $1.3 billion. If Milliman’s projection of the woodwork population is too low, then the state costs would be considerably higher given the 40 percent state cost for them.
Additionally, according to Milliman’s projections, there are about 31,000 enrollees currently covered by Medicaid who would be reimbursed at the 90 percent rate if the state expands.28 These enrollees are individuals currently eligible for Medicaid through the family planning waiver as well as postpartum women.
Nearly 60 percent of funding that states receive from the federal government comes through Medicaid. Such a high level of funding means that states, particularly Medicaid expansion states, are vulnerable to a change in federal fiscal policy that reduces the FMAP. Along with Medicare, Medicaid is the main program responsible for the long-term fiscal imbalance of the federal budget.29 Congress will likely be forced to deal with the significant fiscal pressures that Medicaid is placing on the federal budget within the next decade.
When Congress is forced to pursue long-term deficit reduction, lowering the FMAP for the expansion population will undoubtedly be under consideration. Congress will likely consider a blended Medicaid reimbursement rate, which would reduce the FMAP for the expansion population. Reducing the expansion FMAP has attracted bipartisan support in the past. President Obama included a blended rate proposal in his 2012 budget.30 And numerous congressional proposals have gone further, some phasing out the expansion FMAP entirely. The American Health Care Act, which passed the House of Representatives in May 2017, phased out the expansion FMAP.31
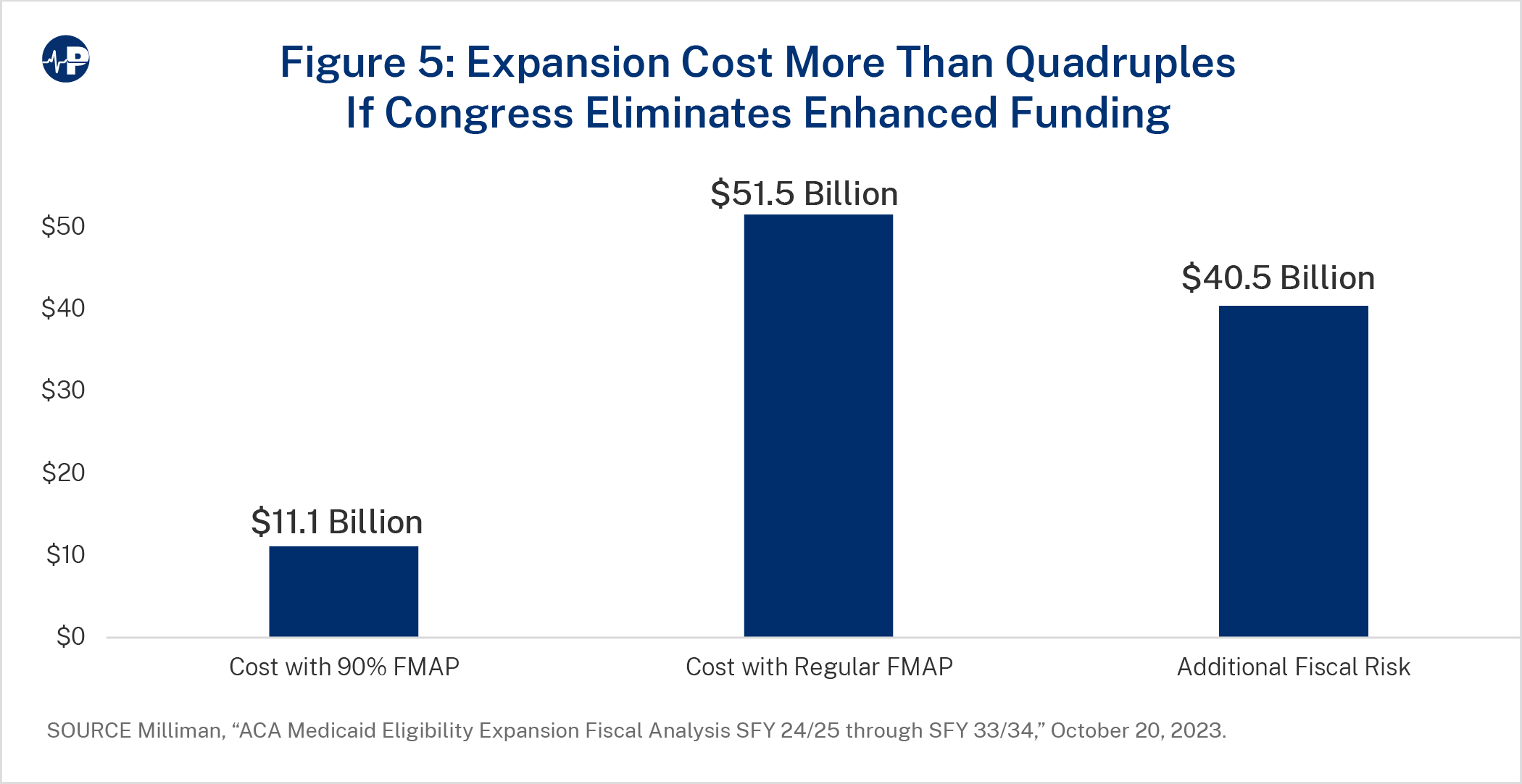
If Congress were to adopt a policy phasing out the expansion FMAP, the cost to Florida for expanding Medicaid would be severe. As a rough estimate using Florida’s standard FMAP, the state share of the expansion population would be $4.9 billion in 2028 and $51.5 billion over a decade.32 Figure 5 contrasts the 10-year costs to Florida of the expansion depending on whether the state receives a 90 percent FMAP or its standard FMAP of about 60 percent. The difference—roughly $40.5 billion over 10 years—is the fiscal risk that Florida assumes if it expands Medicaid.33
Medicaid expansion would also hurt Florida’s fiscal position. According to the state’s long- range financial outlook, the state’s current fiscal situation signals that a “structural imbalance may be emerging, absent any prior corrective actions,” and “based on the results of this Outlook, the Legislature can undertake no more than $130 million of additional recurring expenditures, and no more than $2.3 billion of other one time-time investments in Fiscal Year — 2024-2025 without causing a negative balance in Year 3.”34 According to Milliman, expansion would cost the state an average of $1.4 billion per year over the next decade, over 10 times the $130 million the state warns against undertaking in recurring balances given its current financial situation. In Milliman’s high estimate scenario, the state would need to find a way to pay for an additional $2 billion in additional Medicaid spending or make large cuts to other public priorities.
Importantly, as will be discussed later in the paper, past state expansions have typically resulted in much greater enrollment and spending than projected. If this pattern holds, the costs of the expansion would be about one-third higher than what Milliman projects, and Medicaid expenditures as a share of the state budget would grow to about 43 percent.
There are several key lessons from states that have adopted the ACA Medicaid expansion.
States that adopted Medicaid expansion experienced much greater enrollment in the program than they expected. In March 2016, CBO reported that “the number of people estimated to have been enrolled in Medicaid in 2015 who were made eligible for the program by the ACA was significantly higher than … previously projected.”35 In 2016, Brian Blase (one of this paper’s authors), adjusting for slower state take-up of Medicaid expansion than CBO originally projected, estimated that enrollment was upwards of 50 percent more than what CBO expected when the ACA became law.36
Table 2 contrasts Medicaid expansion enrollment projected by the Urban Institute with actual enrollment.37 Urban’s projections were made in November 2012 and were their expectations of expansion enrollment in 2022. We took actual enrollment from February 2020, the last month before the pandemic (to avoid conflating Medicaid expansion’s effect with the increase in enrollment from the pandemic and policy changes following it). Table 2 also shows the percentage that February 2020 enrollment exceeds Urban’s projections for 2022. The table shows the information for 26 states, including the District of Columbia. We excluded the 19 states that did not expand Medicaid before 2019 and the six states that had expanded their Medicaid programs to cover childless adults prior to the ACA Medicaid expansion taking effect.38
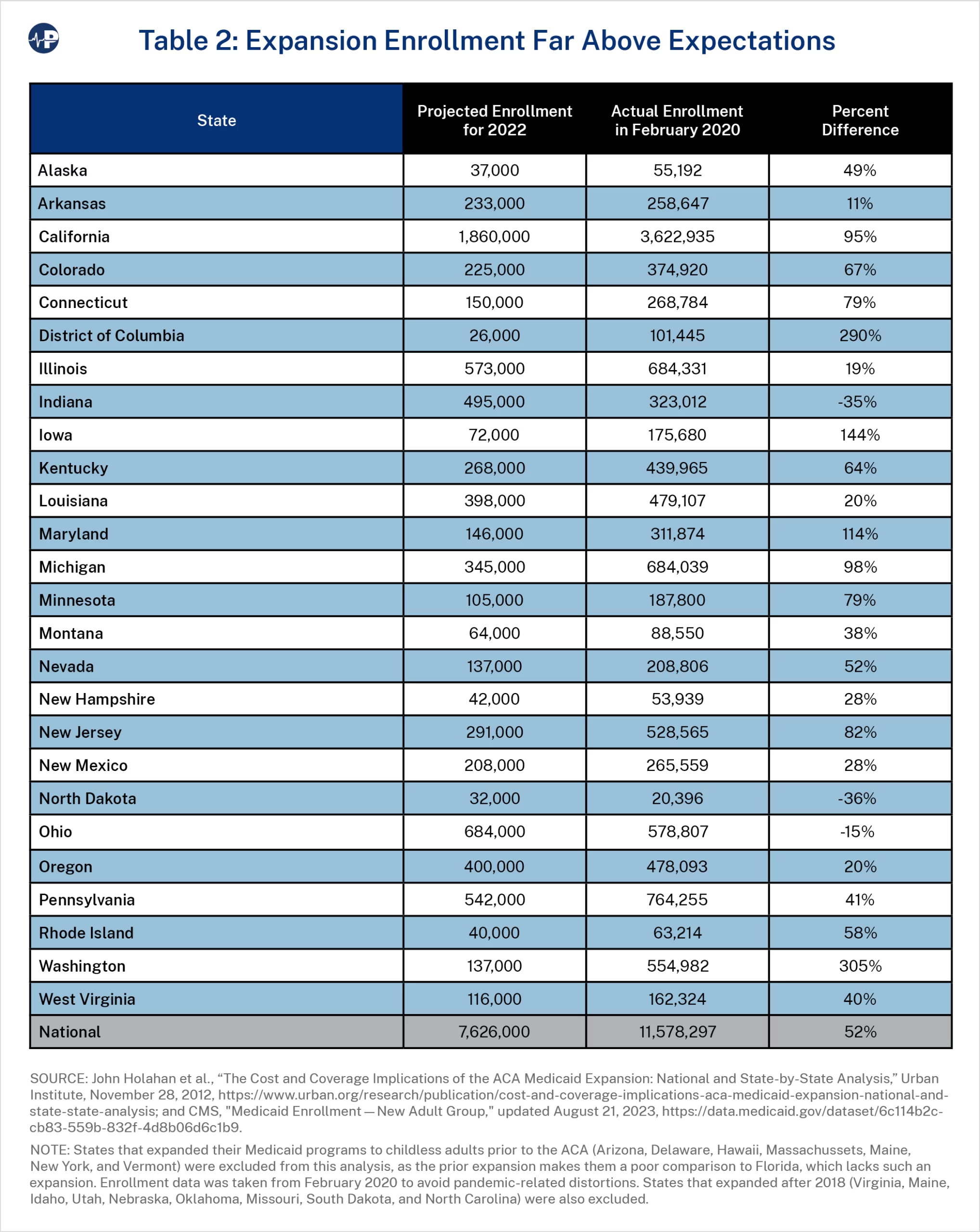
Overall, enrollment exceeded expectations by 52 percent in expansion states. In several states enrollment was much greater than expectations: California (95 percent), Connecticut (79 percent), the District of Columbia (290 percent), Iowa (144 percent), Maryland (114 percent), Michigan (98 percent), Minnesota (79 percent), New Jersey (82 percent), and Washington (305 percent). Given previous state experiences with Medicaid expansion—where enrollment tends to far exceed projections—it is possible, even likely, that the number of people added to Florida’s Medicaid program would be closer to 3.1 million (an amount 50 percent above projections).
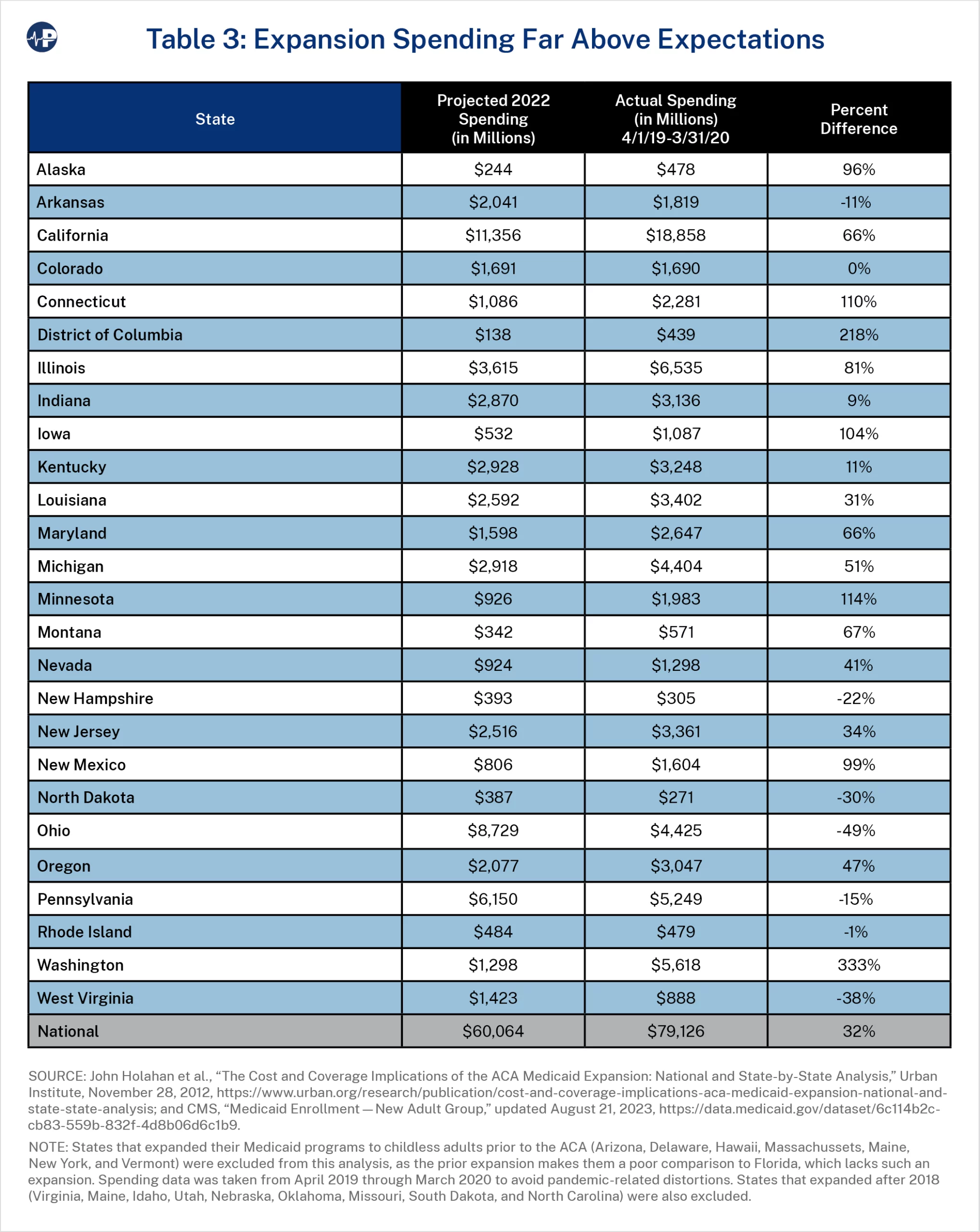
Since expansion enrollment has been so much greater than expected, so has spending. Table 3 contrasts Medicaid expansion spending projected by the Urban Institute with actual spending. Like its enrollment projections above, Urban’s projections were made in November 2012 for the year 2022. The actual expenditure data is from April 2019 to March 2020, so almost entirely prior to the pandemic.39 It also shows the percentage that total spending exceeds projections. Overall, spending exceeded expectations by 32 percent. In several states enrollment was much greater than expectations: Alaska (96 percent), California (66 percent), District of Columbia (218 percent), Connecticut (110 percent), Iowa (104 percent), Illinois (81 percent), Maryland (66 percent), Minnesota (114 percent), Montana (67 percent), New Mexico (99 percent), and Washington (333 percent). Of note, these comparisons use actual spending levels in 2019, while Urban projected spending levels for 2022. If the same year were used for both the projections and actual spending, total spending would likely be considerably more than 32 percent above projections, as spending would have grown between 2019 and 2022 even absent the pandemic-related growth.
Spending has not been higher than expected just because of unexpectedly high enrollment. As Figure 6 shows, per enrollee expansion expenditures have also been much higher than expected.
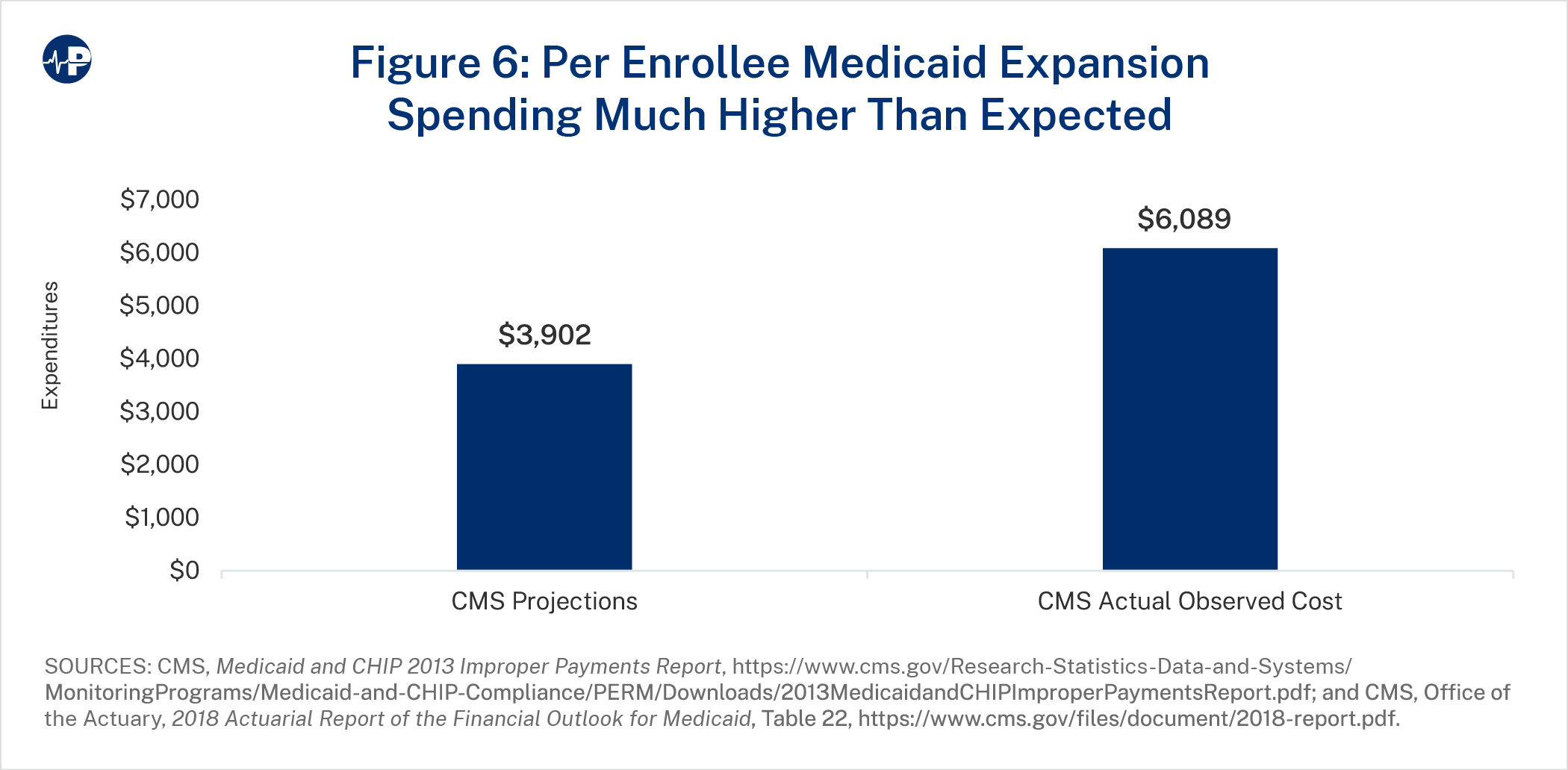
In its 2013 Actuarial Report on the Financial Outlook for Medicaid, the Centers for Medicare and Medicaid Services (CMS) projected that spending per enrollee on the expansion population in 2018 would be $3,902.40 In the 2018 actuarial report, CMS reported that per enrollee Medicaid expansion spending equaled $6,089—or 56 percent higher than what CMS’s actuaries expected prior to the expansion taking effect.41
Much higher-than-expected enrollment and much higher-than-expected spending per enrollee should not have both occurred. The people most eager to enroll in Medicaid should have been the ones with the most expensive health needs. Thus, relatively low enrollment would mean relatively high per enrollee expenses. People who enroll just because of the extensive state and insurer outreach efforts should have relatively low expected medical expenses.
The incentives from the elevated FMAP for the expansion population likely meant that neither states nor insurers were concerned with budget constraints, seeing the expansion as heavily discounted federal money. As demonstrated in California, states set extremely high payment rates for insurers, and insurers reaped windfall profits from the much greater number of people who enrolled in Medicaid than expected.42
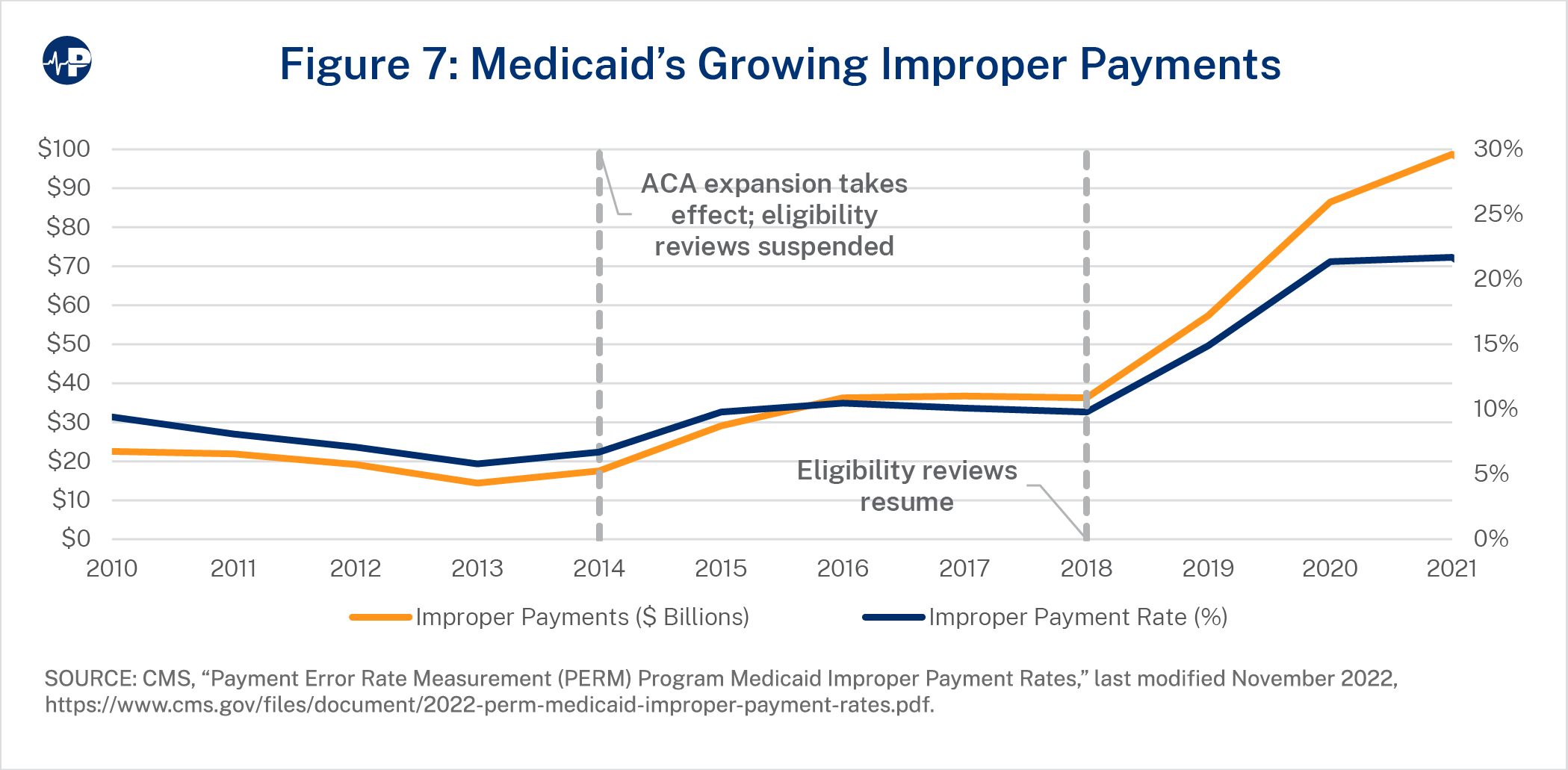
Medicaid expansion has resulted in a massive increase in Medicaid improper payments. In 2013, CMS reported that the national Medicaid improper payment rate was 5.8 percent.43 By 2020, the national Medicaid improper payment rate rose to 21.7 percent—nearly quadrupling the pre-ACA percentage.44 (The actual Medicaid improper payment rate was higher, but CMS paused its audit from April to August 2020 citing the pandemic and did not fully audit one- third of the states for the 2020 report.)45 In dollars, annual federal improper payments increased from an estimated $14.4 billion to $98.7 billion over this period. Figure 7 shows the increase in national improper payments over time. Of note, CMS paused eligibility audits from 2014 to 2017, and because states did not properly review eligibility during that period, improper payment rates were severely understated. Further, as the improper payment rate is an average over three cycles, the 2018 report accounted for only one-third of states having eligibility reviews, and the 2019 report had only two-thirds of states having eligibility reviews.
The expansion of the ACA was the main reason that Medicaid’s improper payments soared. The primary problem is that millions of people who enrolled in Medicaid were ineligible for the program or were put on the program without proper eligibility reviews. According to a fact sheet corresponding to the November 2019 CMS improper payment report:
Medicaid and CHIP eligibility improper payments are mostly due to insufficient documentation to verify eligibility, related primarily to income or resource verification for both situations where the required verification was not done at all and where there is indication the verification was initiated but there was no documentation to validate the verification process was completed, and non-compliance with eligibility redetermination requirements.46
Assuming the trend in Florida’s improper payments mirrors what happened nationally after states expanded, by state fiscal year 2027, improper payments in Florida’s program would grow from $2.5 billion to $11.3 billion.47 Over the first five years of expansion in Florida, improper payments would increase by $52.1 billion in total.
Large Medicaid improper payments are particularly concerning given overwhelming evidence of the low benefit that able-bodied, working-age enrollees receive from the program. According to a 2015 study from economists at MIT, Harvard, and Dartmouth that looked at Oregon’s pre-ACA expansion of the program (discussed further below), “Across a variety of alternative specifications, we consistently find that Medicaid’s value to recipients is lower than the government’s costs of the program, and usually substantially below.”48 The economists estimated that the “welfare benefit to recipients from Medicaid per dollar of government spending range[s] from about $0.2 to $0.4.”49
When states adopt Medicaid expansion, the result is a surge in demand for health care services. The ACA did not contain provisions that increased the supply of health care services or the number of providers. Without an increase in health care supply or increase in health care productivity, the result from a large public coverage expansion is mostly a reallocation of health care services, meaning that some people would face reduced access to care after the expansion. Because Medicaid typically pays lower rates than private insurance and Medicare do, the people most negatively affected from the reduced access to services are traditional Medicaid enrollees.
In a December 2022 paper, Charles Blahous and Liam Sigaud found that Medicaid expansion resulted in less state Medicaid spending on children and the aged and higher spending on non-disabled, working-age adults.50 Contrasting state spending trends from 2013 to 2019 between expansion states and non-expansion states, they found “strong evidence of a shift of financial resources away from certain vulnerable enrollee populations, the most notable being from low-income children.”51 Figure 8 shows the trends in Medicaid per enrollee spending on children in expansion and non-expansion states and shows that spending growth in non-expansion states was three times the growth in expansion states.
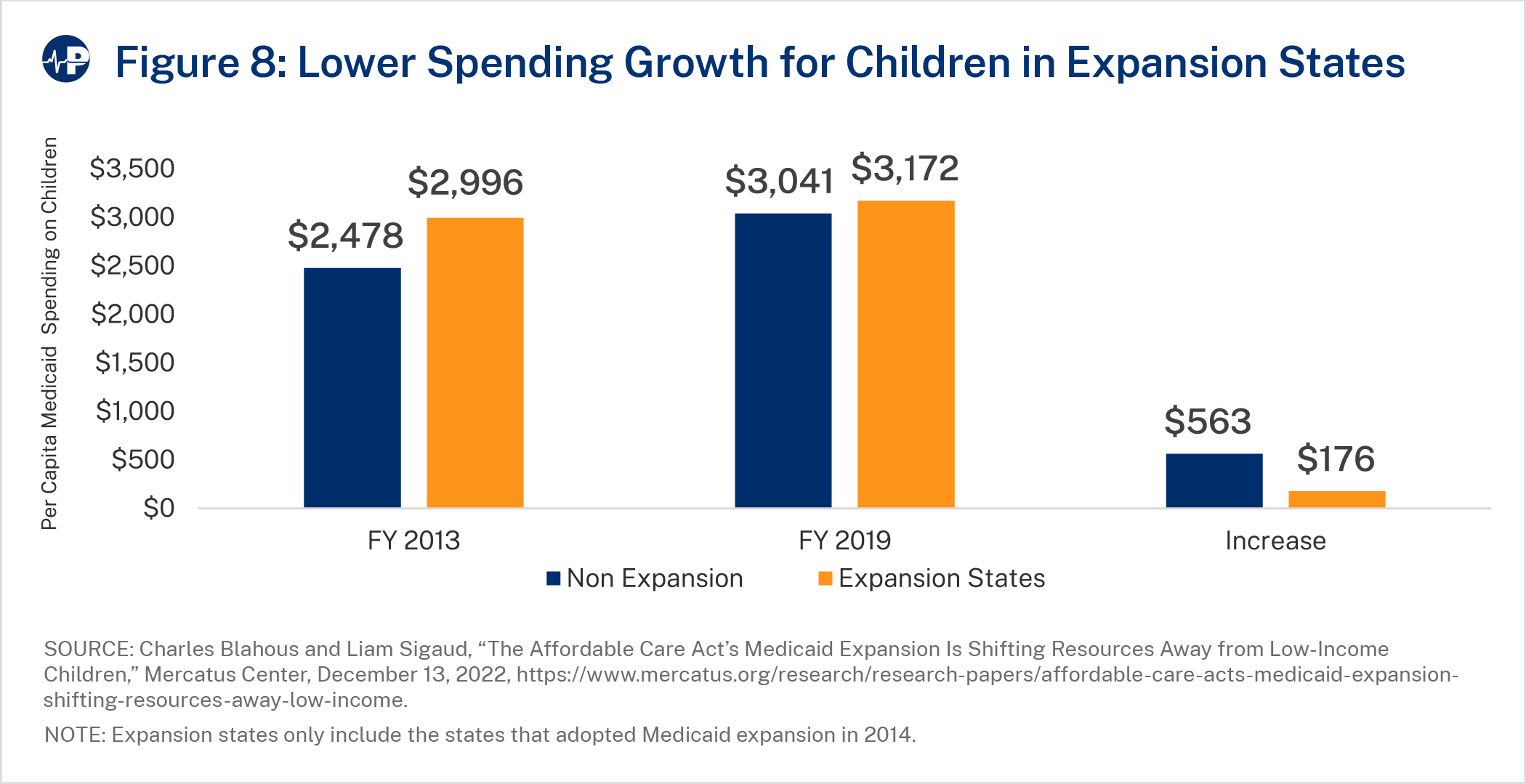
Specifically, Blahous and Sigaud found that “[p]er capita Medicaid spending growth on children in expansion states was less than one-third what it was in nonexpansion states and less than one-quarter of national average per-capita healthcare spending growth.”52 They also found that Medicaid spending growth rates on the aged were much lower than in expansion states and that enrollment of the disabled in Medicaid declined in expansion states. These findings suggest that if Florida chooses to expand, existing Medicaid enrollees—including children, pregnant women, and individuals with disabilities—will have a harder time obtaining medical appointments and will become more reliant on receiving services in the emergency room.
When public programs expand, private health coverage declines. As explained in the next section, private coverage typically provides superior access to care. The amount of crowd- out—or replacement of private coverage with public coverage—depends on several factors, including the degree to which the population targeted for the expansion has private coverage as well as the relative desirability of public coverage versus private coverage. Several studies have attempted to quantify the crowd-out or private coverage from past Medicaid expansions.53
A 1996 paper by economists David Cutler and Jonathan Gruber estimated that Medicaid expansions in the late 1980s and early 1990s were associated with 50 percent crowd-out.54 This means that for every two people who enrolled in Medicaid, one of them replaced private coverage with Medicaid. A 2008 paper from Gruber and Kosali Simon estimated a 60 percent crowd-out rate for Medicaid expansions from 1996 through 2002 for children.55 More recent studies on the crowd-out effect of Medicaid find that crowd-out ranges from 35 percent to 43 percent.56
Medicaid expansion would result in two main sources of crowd-out. First, almost everyone in a household with income between 100 and 138 percent of the FPL who has an exchange plan would lose eligibility for a premium tax credit and replace the exchange plan with Medicaid. These people now qualify for a premium tax credit that typically covers the entire premium for many plans available to them. Second, some people with income between 100 and 138 percent of the FPL would replace their employer plans with Medicaid if the program is expanded.
According to Milliman’s mid-range estimates, if Florida expands Medicaid, 2.09 million people would be added to the program by 2029. Milliman expects a crowd-out rate of 65 percent, meaning that nearly two of three new Medicaid enrollees would replace private coverage with Medicaid.57 According to Milliman, about 1.25 million people would replace exchange plans, and 85,000 people would replace employer plans.58 According to Milliman’s high estimates, Medicaid expansion would add 2.59 million people to the program, with about 1.54 million people replacing exchange plans and more than 100,000 people replacing employer plans.
Some Medicaid expansion supporters hoped that expansion would help people obtain health services, but the evidence suggests that Medicaid enrollees have less access to timely and proper health care services. Importantly, people with private coverage tend to have better access to high-quality providers, so those who replace private coverage with Medicaid can experience a deterioration in their health care treatment as well as their health. Because Medicaid has historically paid relatively low rates for physicians, many providers refuse to treat Medicaid enrollees, forcing numerous Medicaid enrollees to receive a disproportionate amount of non-emergent care in emergency rooms.59 A 2011 study in the New England Journal of Medicine found that researchers who attempted to obtain appointments by posing as mothers of children with serious medical conditions were six times more likely to be denied an appointment if their children were on Medicaid compared to private insurance.60
Prior to Medicaid expansion, many Medicaid recipients could not find doctors to treat them, a problem that expansion would undoubtedly make worse. For example, fewer than one-third of Texas doctors accepted Medicaid patients in 2010.61 In 2011, the New York Times reported on the low access to care faced by Louisiana Medicaid patients.62 One woman remarked, “My Medicaid card is useless for me right now. It’s a useless piece of plastic. I can’t find an orthopedic surgeon or a pain management doctor who will accept Medicaid.”63
Many Medicaid expansion enrollees already struggle to find primary care physicians as well as specialists. One study found that one-third of primary care physicians do not accept Medicaid patients.64 A 2015 survey of primary care providers in 2015 revealed that 45 percent of them were willing to accept new Medicaid recipients, while 94 percent were willing to accept privately insured patients.65 And given the increasing demand for mental health services, it is worth noting that two-thirds of psychiatrists refuse to treat Medicaid patients.66
Medicaid recipients in expansion states significantly delayed medical care because no appointment was available or because waits times were too long.67 Another study found that Medicaid expansion was related to a significant increase in the amount of time for ambulances to respond.68
A meta-analysis published in Inquiry in 2019 reviewed 34 studies that contrasted health care access between Medicaid recipients and those with private coverage.69 They found that Medicaid patients were 1.6 times less likely to schedule a primary care appointment and 3.3 times less likely to schedule a specialty appointment than people with private insurance. The study also contrasted appointment accessibility for Medicaid patients before and after Medicaid expansion, finding that expansion was associated with less ability to secure appointments. In studies prior to expansion, Medicaid patients were half as likely as someone with private insurance to get an appointment. In the studies after expansion, Medicaid patients were one-third as likely as someone with private insurance to get an appointment.
Some Medicaid expansion supporters believe that expansion would help hospitals, but expansion’s effects on hospital finances are unclear. On the one hand, expansion reduces the amount of uncompensated care that hospitals provide.70 On the other hand, the crowd-out of expansion results in some people with Medicaid instead of private insurance. Since Medicaid pays 60 percent of what private insurance pays on average, hospitals lose money when enrollees shift from private plans to Medicaid.71
According to a study from the Foundation for Government Accountability (FGA), between 2013 and 2016, Medicaid shortfalls—or the gap between the Medicaid payment rate and hospitals’ reported costs for providing services for Medicaid enrollees72—at hospitals in expansion states grew by roughly 50 percent.73 The study found that hospital profit margins increased in non-expansion states while declining by 10 percent in expansion states.
FGA also found that nearly 50 hospitals, including more than a dozen rural hospitals, closed after Medicaid expansion was implemented. Furthermore, only 5 percent of hospitals that closed in non-expansion states cited a lack of Medicaid expansion as a reason for their closure.
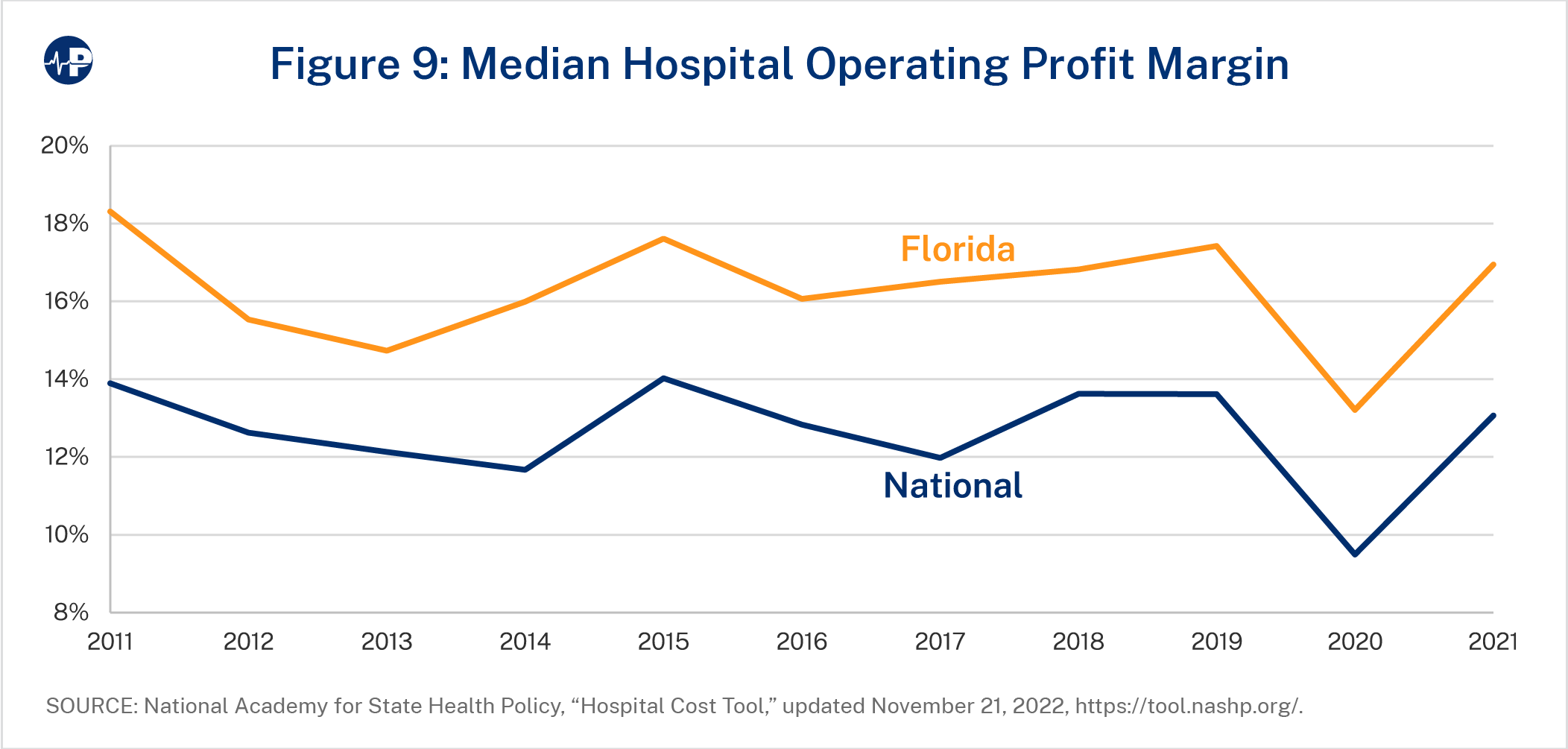
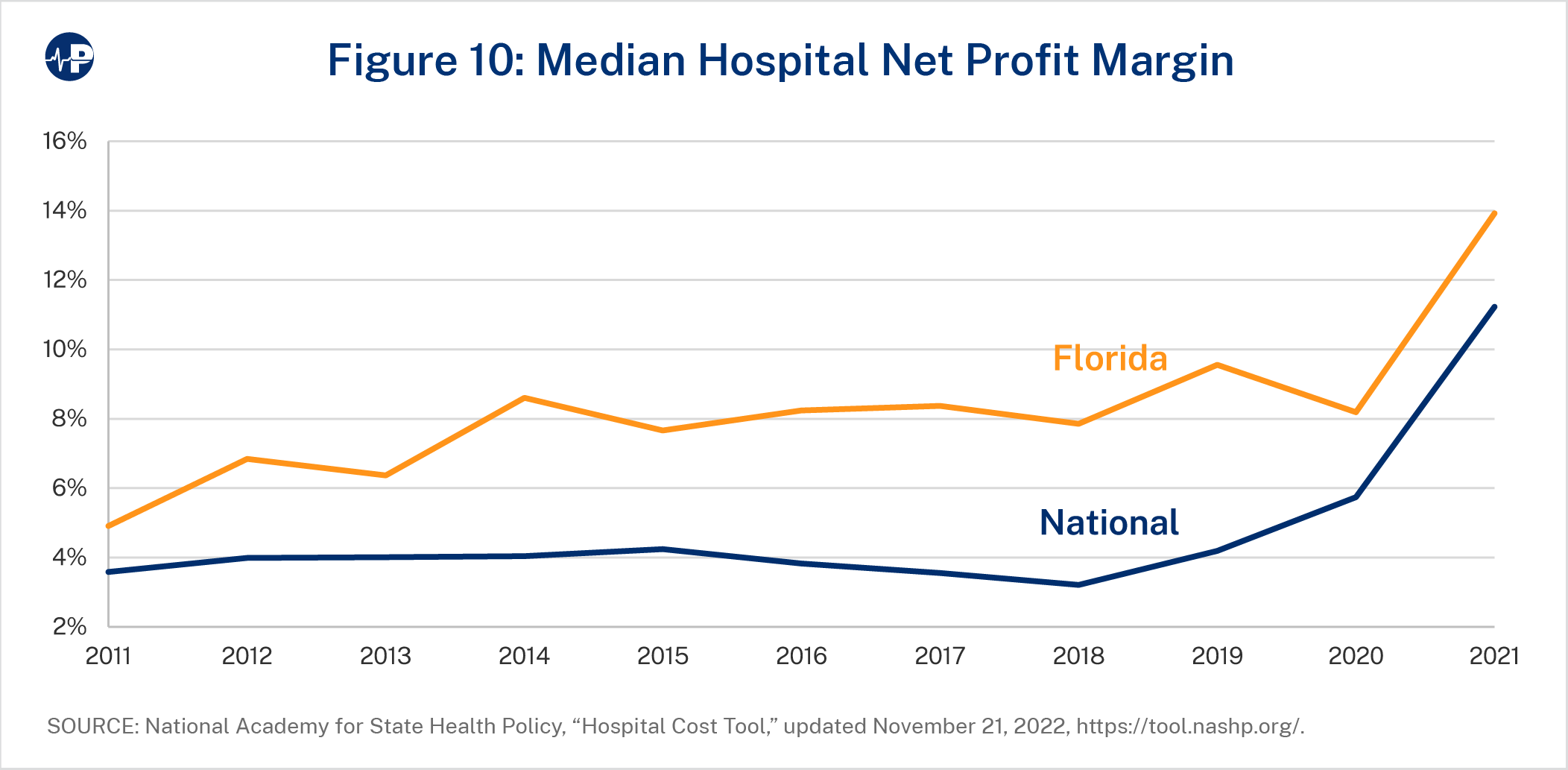
In terms of financial health, both Florida hospitals’ operating margins and net profit margins are well above the national averages.74 As Figure 9 and Figure 10 show, Florida hospitals have exceeded the national median on both metrics every year since 2011.75 Thus, even if Medicaid expansion were a financial positive for Florida hospitals, these funds would be unnecessary.
Medicaid expansion proponents hypothesized that expansion would reduce emergency department utilization. Then-President Barack Obama and then-House Speaker Nancy Pelosi said that expansion would result in increased access to primary care and less reliance on emergency rooms.76 This theory has been invalidated by real-world experience. It turns out that Medicaid expansion resulted in a surge of emergency room (ER) utilization, often for non-emergent care. Crowding ERs for non-emergent care takes resources away from people who need emergency services.
In 2008, Oregon expanded Medicaid to a set number of enrollees and choose to allocate the limited number of spots through a lottery. Only people who won the lottery and returned the proper paperwork were enrolled in Medicaid. The lottery design allowed researchers to compare health care utilization and outcomes between those who enrolled in Medicaid and those who did not, avoiding many of the methodological problems that inhibit observational studies from finding causal outcomes. The Oregon experiment found that Medicaid coverage significantly increased ER use, particularly for non-emergent care.77
A Brookings Institution study found a 20 percent increase in hospital use for the newly insured, with the increase primarily occurring through “outpatient visits to the emergency department for conditions that might have been deferrable and treatable outside of the emergency department.”78 After Medicaid expansion in Arkansas, a study of Blue Cross enrollees found that Medicaid expansion enrollees used the emergency room at five times the rate of other Blue Cross members and were less likely to use their primary care physicians.79
Many studies correlate different types of health coverage with access to health care and health outcomes. Most of these studies shows that Medicaid patients have worse access and worse health outcomes than the privately insured do.80 One study assessing outcomes from 900,000 major operations in the United States found that Medicaid patients were twice as likely to die in the hospital as were people with private insurance and 13 percent more likely to die in the hospital than the uninsured were.81
The studies that link Medicaid with poor health outcomes are generally observational studies. With observational studies, it is possible that unobservable factors—and thus uncontrollable factors—that are different between Medicaid patients and patients with other coverage explain at least part of the relatively poor health outcomes of Medicaid patients. Regardless, observational studies can provide information about why Medicaid recipients’ outcomes are likely to be worse. For example, Medicaid recipients are often assigned to less-experienced surgeons, and surgeon experience is strongly related to surgical outcomes.82
Results from the Oregon Medicaid experiment found that gaining Medicaid increased health care utilization, as measured by hospital admissions, outpatient visits, ER use, and medications.83 While Medicaid enrollment improved self-reported health, it did not produce actual physical health benefits. There was no significant improvement on any of the three measures of physical health used in the study—blood pressure, cholesterol, and blood sugar.84 It turns out that gaining Medicaid may have had the adverse health effect of increasing tobacco use.85 Medicaid enrollment was associated with improvements in mental health.
A different study contrasted smoking prevalence and past-year quit attempts in expansion states versus non-expansion states.86 While there was some short-term evidence of reduced smoking prevalence in the first two years in expansion states, those effects were not maintained over time. Plus, Medicaid expansion had no effect on quit attempts in either the short or long terms.
Importantly, the results from the Oregon Medicaid experiment essentially confirm the results from the famous RAND health insurance experiment from decades earlier: People with more generous health insurance utilize more health care, but the additional health care does not translate into improved health outcomes.87
Large public health insurance expansions do not just influence the access to care and utilization of health care services for those who gain coverage. They also produce general effects on people who do not change coverage status. The large public health insurance expansion leads to a surge of demand for medical care but, with a relatively fixed supply of care, causes a reallocation of health care services. The reallocation of services can reduce access to services for people who get a higher marginal benefit from health care services than for those who gain coverage under the expansion. As mentioned above, studies show Medicaid expansions relate to an increase in wait times for specialty care and increase in ambulance response time.
Pre-ACA, Tennessee significantly expanded Medicaid in an initiative named TennCare. The number of Tennesseans covered by Medicaid soared from 900,000 to nearly 1.5 million between 1993 and 1995.88 TennCare was not associated with a significant change in utilization overall—evidence supporting a relatively fixed amount of health care supply and a resulting reallocation of services from Medicaid expansion. Tennesseans reported worse health than did people in Tennessee’s neighboring states after TennCare.89 After TennCare, fewer individuals, particularly women, received regular check-ups with their physicians.90 Perhaps most importantly, the mortality trends in Tennessee were worse in the four-year period after TennCare’s enactment than in all eight of Tennessee’s neighboring states (and the trends were similar between Tennessee and its neighboring states in the pre-expansion period).91
In a 2020 paper, Blase and David Balat assessed mortality trends for non-elderly adults in expansion and non-expansion states after the enactment of the ACA. Across the United States, life expectancy declined for three straight years from 2014 to 2017.92 Similar to the TennCare experience, mortality worsened in expansion states relative to non-expansion states. States that performed the worst were states that expanded their Medicaid programs after January 1, 2014, but before mid-2016. Part of the reason for the mortality differences could be that Medicaid expansion states experienced a far greater increase in drug overdose deaths from opioids after 2013 than did states that did not adopt the expansion.93 As reported by Sam Quinones, real-world experiences suggest that Medicaid exacerbated the opioid crisis by making it easier for people to obtain opioid prescriptions, causing opioids to flood local areas.94
There are several reasons why large Medicaid expansions to adults yield disappointing outcomes. First, there is a crowd-out of private coverage, which is likely superior in delivering improved health. Second, the expansion largely reallocates existing health care services, and likely does so by reducing access to care for people with more pressing health needs. Third, the uninsured obtain almost as much as health care as do people with insurance, with one study estimating that the average uninsured person utilizes 80 percent as much health care as do the privately insured.95
More recently, a Mercatus Center study examined the self-reported mental health of continuously covered near-elderly Medicaid enrollees. It found that Medicaid expansion caused an 11 percent increase in depression scores among the original enrollees, with particularly negative effects among women and individuals with disabilities. According to the conclusion:
Our evidence is most consistent with the hypothesis that Medicaid expansion put strain on the healthcare systems in expansion states, making it difficult for some already-enrolled beneficiaries to access psychological or psychiatric treatment. This could explain why the subgroups most affected in our sample are residents of nonmetro areas—where access to care is often more limited—and in areas with newly developed shortages of mental health professionals.96
In a 2019 paper, Harvard economists Nathaniel Hendren and Ben Sprung-Keyser examined 133 policy changes over the past half-century to estimate the “marginal value of public funds.”97 This marginal value is a measure of the investment return of the government program. According to their study, spending on the health and education of low-income children had the highest returns, boosting education achievement and income. For Medicaid expansions to children, Hendren and Sprung-Keyser estimated that each $1 of initial spending was fully repaid and that the policy returned an additional $0.78 to the government. Thus, the evidence suggests that House Bill 121, which Florida enacted last session and expanded income eligibility for the Florida KidCare program, will have a net benefit for the state’s population.
However, because the ACA expansion was geared toward able-bodied, working-age adults, their work is most important in this context as they found that additional health care spending on adult populations had among the worst returns of all programs. In fact, these rates of return were generally negative, significantly reducing incentives to work. In their 2020 paper, Blase and Balat wrote, “It is also worth noting that large coverage expansions likely have a poor return on investment because there is already a myriad of government programs to help lower-income people obtain medical care, including requirements that hospitals render emergency services regardless of ability to pay, federal programs for uncompensated care, federally qualified health centers, and many block grants for low-income population needs.”98
Expanding Medicaid almost certainly increases pharmaceutical fraud and abuse, including consumers receiving drugs illegally, providers fraudulently prescribing drugs, and pharmacies filling illegal prescription orders. A 2015 Government Accountability Office report found that over 16,000 drug recipients shopped with five or more doctors in order to receive $33 million in antipsychotics or respiratory medications.99 In 2017, the Department of Health and Human Services Office of the Inspector General outlined certain common scenarios that take place within the Medicaid program. For example:
A doctor bills the Medicaid program (directly or through a contract with a managed care entity) for an office visit with a Medicaid beneficiary and writes a prescription, but there is evidence that the doctor fabricated the diagnosis to permit the beneficiary to misuse the pharmaceutical or to divert it for financial gain….
An employee of a facility steals drugs from the facility that are paid for by Medicaid and intended to be administered to a Medicaid beneficiary residing in the facility. The drugs are then diverted for financial gain or other illicit purposes.100
In 2021, the Department of Justice charged an owner of a pharmacy in New York with fraud when he was caught paying kickbacks and bribes to customers worth over $6.8 million in Medicaid and Medicare reimbursements.101 In 2022, the Texas Office of Investigative Government found that a pharmacy was fraudulently billing Medicaid to the tune of over $1.3 million.102 And, in 2022, the State of Washington fined Centene, a large Medicaid managed care organization that serves most state Medicaid programs, $19 million because it failed “to disclose true pharmacy benefits and services costs.”103 Iowa also reached a $44 million settlement with the same provider for overbilling for pharmacy and prescriptions.104
In 2015, CBO wrote that the ACA “will make the labor supply, measured as the total compensation paid to workers, 0.86 percent smaller in 2025 than it would been in the absence of the law…. The labor force is projected to be about 2 million full-time equivalent workers smaller in 2025 under the ACA than it would have been otherwise.”105 CBO estimated that the Medicaid expansion would reduce new eligible individuals’ labor force participation by almost 4 percent. CBO referenced many studies that examined previous changes in eligibility for public health insurance coverage in its work, but it has yet to publicly update its estimates.106
Since CBO’s estimates, other studies have found that Medicaid expansion resulted in negative effects on labor supply. One study found that from 2014 to 2016, Medicaid expansion reduced employment in expansion states by 1.6 percent.107 A second study found that public insurance coverage had “sizable and statistically meaningful reduction in employment, with an estimated effect size of just over 5 percentage points” in Wisconsin. Another study found that total employment decreased by 1.2 percent one year after the expansion of Medicaid.108 A fourth study examined Medicaid expansion’s effect on labor supply decisions of older workers and found that, with Medicaid expansion, insured workers without retirement health insurance decreased full-time work by 7.1 percent.109 There have been some studies that have found smaller or negligible effects on labor supply.110
Florida’s unemployment rate is exceptionally low—2.7 percent in August 2023—quite a bit lower than the national unemployment rate of 3.8 percent.112 Expanding Medicaid would reduce Florida’s advantage. Based on the trends in other states, expansion could reduce employment in Florida by up to 2 percent, which translates to about 222,000 fewer workers.
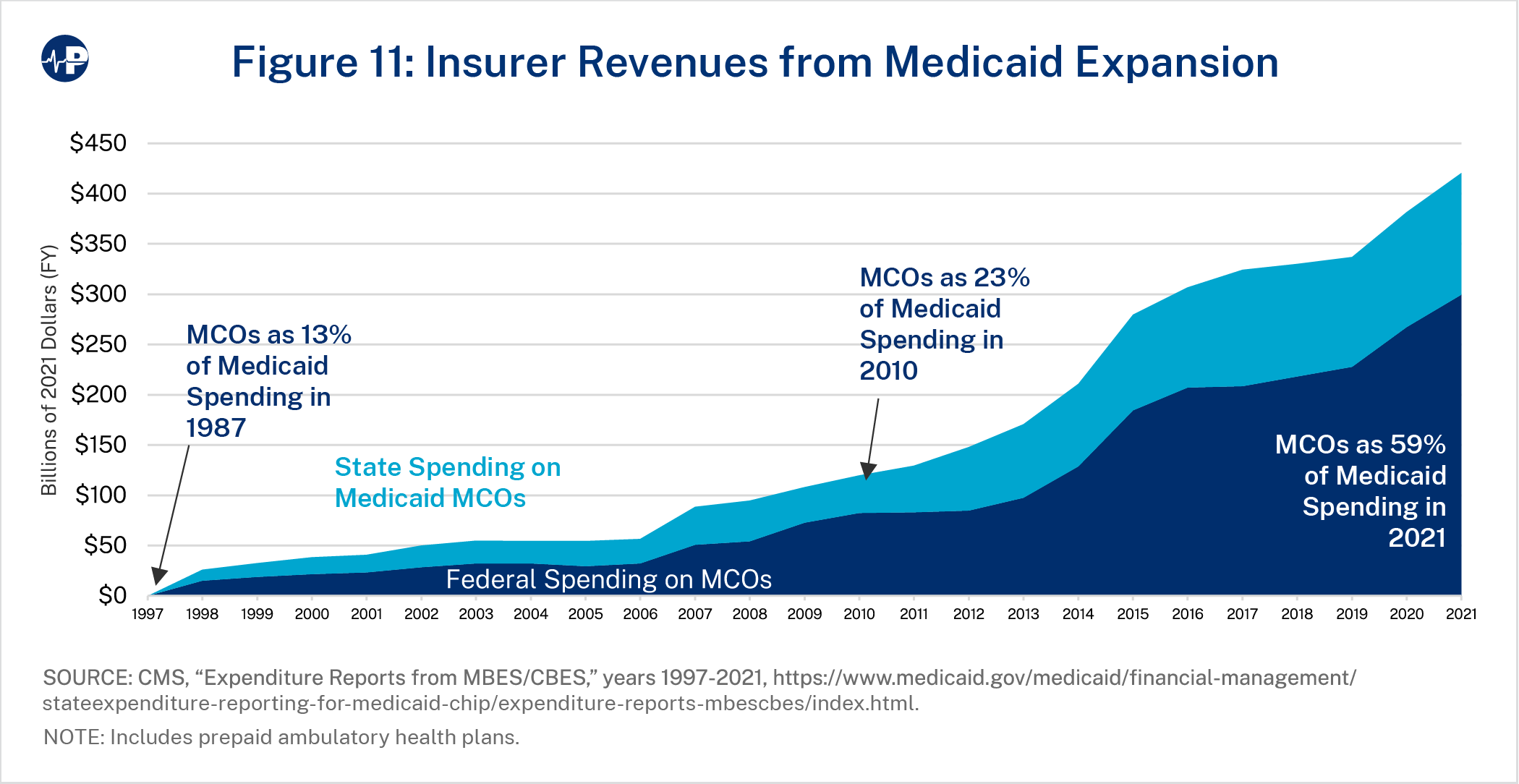
This surge in Medicaid enrollment and spending has drastically increased revenue for insurers participating in Medicaid. Over 70 percent of all Medicaid recipients—and a much higher percentage of ACA expansion recipients—are enrolled in managed care.112 Under this structure, the government pays insurers a monthly amount regardless of whether the enrollee utilizes any health care services at all or whether they are even eligible for the program. Figure 11 shows the national increase in Medicaid managed care expenditures. Medicaid spending through managed care organizations (MCOs) has quadrupled after the ACA in inflation-adjusted dollars—up from about $100 billion in 2010 (the year the ACA was enacted) to $420 billion in 2021 (59 percent of program spending).113
According to Milliman’s estimates, if Florida adopts the ACA’s Medicaid expansion, Medicaid enrollment would increase by between 47.4 percent and 59.8 percent, and Medicaid spending—inclusive of federal funds—would increase by between 30.4 percent and 42.8 percent.
Because enrollment and expenditures significantly exceeded projections in expansion states, these estimates are likely to be lower than what would actually occur. It is possible, even likely, that Medicaid enrollment would increase by more than 3 million people and more than 30 percent of Florida’s residents would be enrolled in Medicaid after expansion. The number of Florida workers per Medicaid recipient would decline by approximately 40 percent—from about 2.5 to only about 1.5 if the state expands Medicaid.
Existing Medicaid growth already eats up a larger portion of state budgets, driving the growth of government and crowding out other public priorities while creating pressure for tax increases. Even without expansion, Medicaid spending growth in Florida outpaced the growth of other government areas by a ratio of nearly six to one since 1988.
Expansion would reduce the number of people without health coverage, but nearly two-thirds of new Medicaid enrollees would simply replace private coverage, which tends to cover more hospitals and doctors, as Medicaid pays lower rates.
In addition to the much higher government expenditures and crowd-out of both other public priorities and private coverage, based on the experiences of other expansion states, expansion would create several ill effects. Expansion results in an explosion of improper payments, longer wait times for medical appointments and ambulance response times, and a surge of emergency room use for non-emergent services. Expansion also takes resources from existing Medicaid enrollees—particularly children and people with disabilities. States saw a reduction in providers accepting new Medicaid patients after expansion. Florida Medicaid enrollees, some of whom may already struggle to obtain appointments, would find it increasingly difficult to find providers after expansion. Studies show that Florida’s decision to focus Medicaid on lower-income children and people with disabilities has been extremely prudent.
The Oregon Medicaid experiment showed that gaining Medicaid coverage did not lead to physical health improvements for able-bodied, working-age adults. And because expansion results in the displacement of services for other people in the state, expansion has not led to population health improvements and possibly worsens population health. Expansion states had worse mortality trends from 2013 to 2017 than did non-expansion states, driven by greater opioid overdoses.
Florida hospitals have above-average profitability now and certainly do not need to become more dependent on government revenue. Moreover, it seems that expansion fails to meaningfully help hospitals’ finances or stem hospital closures. And expansion would also likely reduce labor force participation and work.
Finally, despite all these drawbacks, Florida lawmakers may be tempted by the large share of the expansion spending covered by the federal government. This has led most other states to expand Medicaid. Importantly, the 90 percent reimbursement rate is unsustainable given the deteriorating fiscal position of the federal government with large and growing budget deficits. President Obama’s budget reduced the enhanced reimbursement rate for the expansion population, and in 2017 the House of Representatives passed legislation completely phasing out the enhanced rate. Thus, if Florida adopts Medicaid expansion, the state would realistically bear a much greater share of the costs over time. If Congress phases out the enhanced rate for the expansion, Florida would be on the hook for an additional $40.5 billion over the next decade. Adopting expansion would threaten Florida’s favorable fiscal climate (low taxes and low spending) that has made the state so welcoming for families and businesses.
Note: Florida contracted with Milliman to estimate the impact of Medicaid expansion. Other than Paragon citing Milliman’s estimates, Milliman was not involved with the creation of the Paragon report and has no position on whether Florida should expand Medicaid. Using the Milliman report to provide context to the costs of Medicaid expansion should not be viewed as Paragon’s endorsement or Paragon taking a position on the methods in
the Milliman report.



