
Gary D. Alexander
A nationally recognized health services expert and government reformer, Gary D. Alexander is head of the Medicaid and Health Safety…
Reforming Government, Empowering Patients
Navigation
This paper outlines strategies for states to efficiently clean up their Medicaid rolls post-COVID-19 by prioritizing the removal of ineligible enrollees, leveraging enhanced federal funding, and providing recommendations to ensure resources are preserved for those truly in need, amidst a backdrop of nearly 20 million potentially ineligible enrollees due to pandemic-era enrollment policies.
During the Obama and Biden administrations, the federal government relaxed Medicaid eligibility requirements, making it easier for millions of ineligible individuals to access the program and more challenging for states to verify applicant information and ensure that only those eligible were enrolled.1 This has contributed to the program’s significant expenditure growth and surge of improper payments over this period. Further, coverage of those who do not qualify for Medicaid crowds out private coverage—particularly employer-sponsored insurance—and shifts costs to taxpayers.2 All of this depletes resources for more vulnerable populations that need a safety net. Prior to the COVID-19 public health emergency (PHE), Medicaid’s improper payment rate already exceeded 20 percent, or nearly $100 billion in federal misspending annually.3 The high improper payment rate was driven by improper eligibility reviews, largely resulting from the incentives for states to enroll people as eligible under the Affordable Care Act (ACA) expansion to obtain a higher federal reimbursement.4 Congressional action at the beginning of the COVID-19 pandemic made the problem worse.
Through the Families First Coronavirus Response Act, Congress offered states enhanced Medicaid matching funds (a 6.2 percentage point boost for traditional Medicaid enrollees) for the duration of the PHE so long as states did not make eligibility reductions or remove ineligible enrollees from the program. While states had the option to not take the funding or to opt out early, all states accepted the funds and did not remove ineligible Medicaid enrollees for more than three years. The continuous coverage provisions after the precipitous employment decline led to many millions more people on Medicaid who returned to the workforce relatively quickly. As a result, nearly 20 million people now have two sources of coverage, with the most common being employer coverage and Medicaid.5
The congressional spending bill passed at the end of 2022 changed the terms of this agreement with states. As of April 1, 2023, states are allowed to resume full eligibility reviews without the risk of losing enhanced federal funding. States are incentivized to start doing redeterminations as quickly as possible as federal funding has also begun ratcheting down and will continue dropping throughout the remainder of the year.
Ultimately, Medicaid misspending harms Americans by taking limited resources from those who rely and depend on these programs—reducing their access to care. Many of them, such as low-income children, pregnant women, individuals with disabilities and the elderly, need Medicaid to finance their medical services.
Medicaid is the nation’s largest public welfare program, costing nearly $800 billion in federal and state funds annually. Medicaid is the largest spending category in state budgets.6 The PHE’s continuous coverage policy drove enrollment even higher, adding nearly 20 million people to Medicaid and creating many program integrity issues.7 Medicaid now has more than 86 million enrollees.8 Approximately 18 million of these recipients are likely to be ineligible for Medicaid.9 An alternative enrollment methodology by the Centers from Medicare and Medicaid Services (CMS), which includes people enrolled in limited benefit plans and counts people enrolled at any time during each month in the quarterly reporting period, suggests that enrollment was around 94 million people in September 2022.10
Pre-pandemic data also showed that one in 10 Medicaid recipients were transient and changed addresses often.11 Movement to another state would result in ineligibility within the previous state, a problem that has not been corrected since early 2020 as states have not reviewed eligibility. The Public Assistance Reporting Information System (PARIS), which assists eligibility workers nationwide to identify recipients with multi-state enrollment, was suspended during the PHE because redeterminations were halted.12 A recipient who is enrolled in Medicaid in multiple states that both use managed care organizations (MCOs) means that two MCOs are receiving capitation payments for this one recipient.13 An analysis from the Urban Institute estimates that 99 percent of individuals expected to be removed from Medicaid through the redeterminations will be eligible for employer-based coverage, ACA exchange subsidies, or other taxpayer-funded coverage such as the Children’s Health Insurance Program (CHIP).14
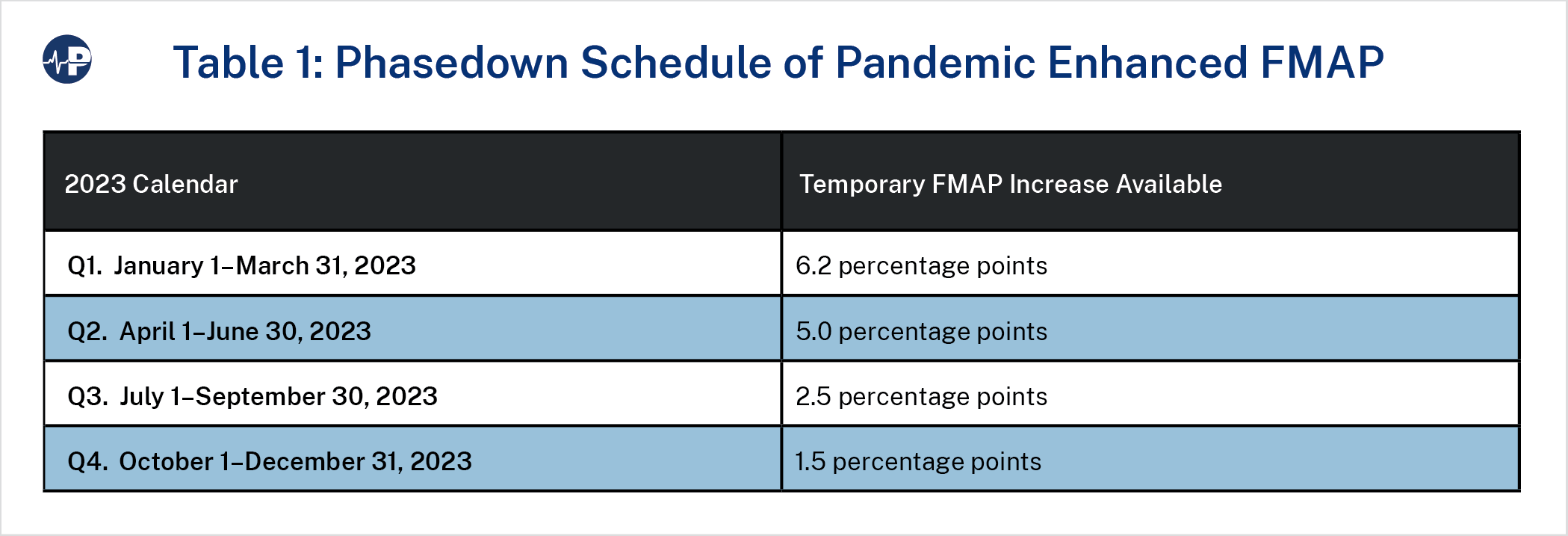
The enhanced funding associated with the continuous coverage requirement (a boost in states’ federal medical assistance percentage, or FMAP) has already begun phasing down and will end entirely at the end of 2023. As of April 1, the enhanced federal funding dropped from 6.2 percentage points to 5.0 percentage points. On July 1, it will drop again to 2.5 percentage points and to 1.5 percentage points in the fourth quarter of the year. The phase-down and end of the enhanced FMAP means states have an incentive to ensure that as many ineligible enrollees are removed by the end of the year. States, therefore, need to quickly create a roadmap that removes the ineligible enrollees expeditiously and preserves resources for the truly needy.
The reinstated eligibility redetermination process will present states with some challenges due to the myriad of newer eligibility rules that make it easier to attain and maintain eligibility, potential staffing shortages, and many recipients’ unknown or unreported mailing addresses.16 These rules, which impose burdens on states that must be met before anyone can be removed from Medicaid, are intended to ensure that Medicaid-eligible recipients stay on the program and to protect those who might be incorrectly removed. These new rules are a reversal from longstanding eligibility rules, including in President Obama’s first term, which allowed states to perform eligibility reviews and verifications every six months or even more often, required a minimum of one such review per year, and included strict income verification guidelines. Moreover, those removed from the program incorrectly can easily regain access to Medicaid. The totality of these new rules and enrollee protections should shield states from accusations of moving too fast to ensure that only those eligible are enrolled. For example, before anyone can be removed, states must:
For individuals who might be incorrectly removed, there are also many protections, including but not limited to:
These are just some of the protections in place that protect Medicaid enrollees from wrongful disenrollment. Some states are even taking additional steps to minimize the chance of disenrolling eligible individuals.25 Overall, existing Medicaid rules and regulations provide ample protection for enrollees, and misguided fear should not deter states from moving swiftly to conduct redeterminations and best ensure taxpayer funds are preserved for those eligible.
Almost all current Medicaid enrollees who do not meet eligibility requirements either already have other coverage or will qualify for it once they lose Medicaid. According to the Urban Institute’s estimates, 18 million people will lose Medicaid once redeterminations are completed.26 Nearly 10 million of them will transition to employer coverage, with many of these individuals currently dually enrolled in employer coverage and Medicaid. According to Urban, more than 3 million children will transition from Medicaid to CHIP, and 1 million people will move to nongroup coverage. Additionally, Urban estimates that 40 percent of those disenrolled who would lack coverage will qualify for low- or no-cost coverage on the ACA insurance exchange, which is heavily subsidized by taxpayers. Moreover, some people who are eligible for programs do not enroll. According to an earlier Urban study that focused on eligibility for other programs for those no longer eligible for Medicaid, only 1 percent of removed enrollees will not qualify for other forms of subsidized coverage, including employer coverage, when they lose Medicaid eligibility.27
Many improperly enrolled individuals are also likely now to be enrolled in multiple states. For example, the Medicaid CHIP Payment and Access Commission found pre-pandemic that 6 percent of enrollees were enrolled in multiple states.28 These individuals should be removed from states they no longer reside in but could retain eligibility in their current states, assuming they meet other eligibility criteria.
Despite some misimpressions, there are not any negative repercussions to states for quickly processing redeterminations. In guidance on how to re-instate the redetermination process, CMS recommended that states “initiate no more than 1/9 of their total caseload of Medicaid and CHIP renewals in a given month during the unwinding period.”29 However, this timing is not a requirement. Further, states are not at risk of losing the enhanced funding sooner than the end of the year if they move more quickly so long as they comply with other federal requirements.30
As discussed, states have an incentive to move quickly, because the enhanced federal funding has already been reduced and will expire at the end of 2023. Indeed, the longer states wait to remove ineligible enrollees from the Medicaid rolls, the more they will pay out of their own budgets to cover them.
Although Arkansas did not remove ineligible enrollees during the PHE, the state continued doing regular eligibility reviews throughout the past three years. This has allowed the state to update and collect data on existing enrollees, flag enrollees who had subsequently become ineligible, and verify that they had reliable contact information for enrollees. This proactive work has made it significantly easier for the state to resume the full redetermination process.
According to the Arkansas Department of Human Services (DHS), as the state begins preparing for redeterminations, it is prioritizing “those whose coverage has been conditionally extended due to the PHE.”31 In other words, because state workers have been consistently reviewing cases for the past three years, they know which enrollees lost eligibility but were extended nonetheless because of the continuous eligibility requirements.
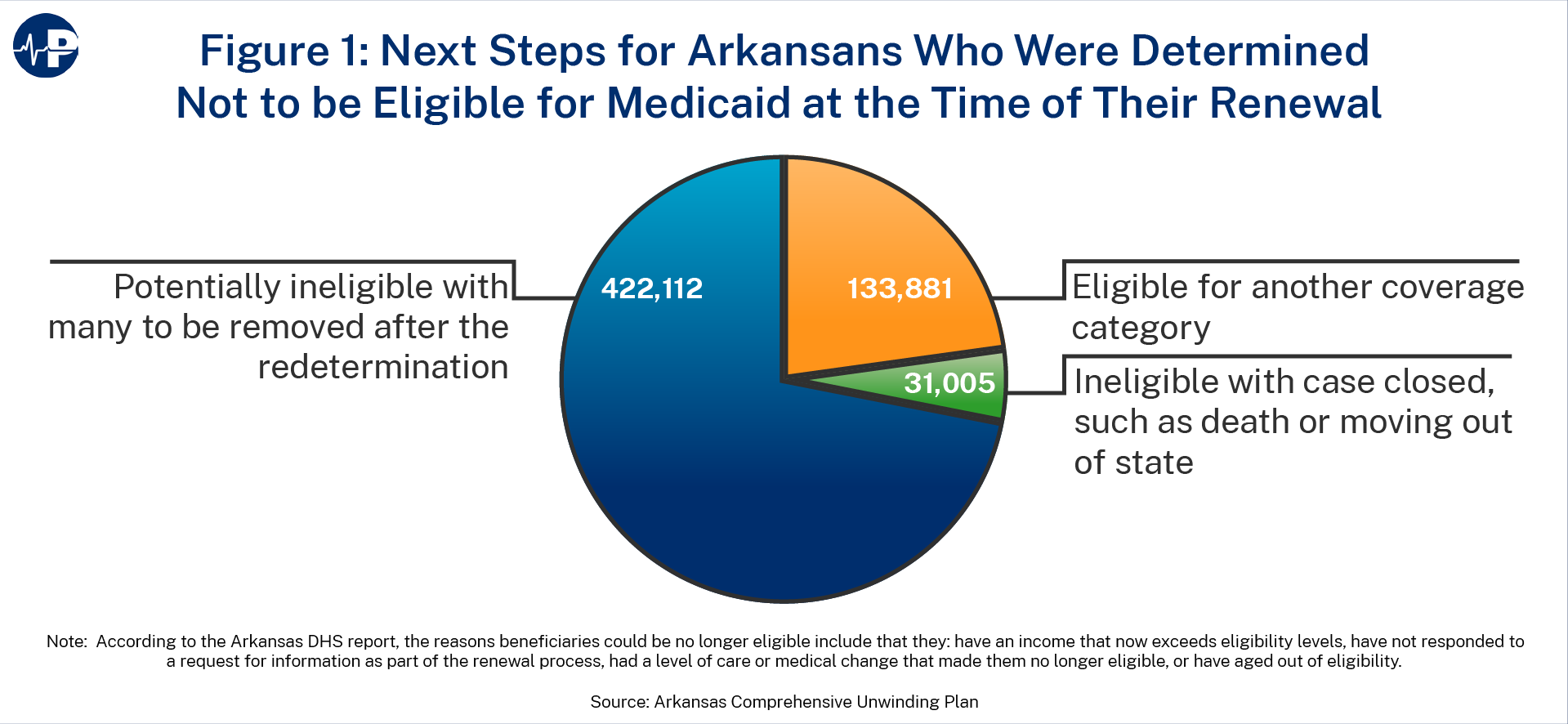
In January 2023, Arkansas began connecting with long-term care facilities and conducting redeterminations. This population is perhaps the least likely to face eligibility changes and also requires the least amount of follow-up for verification. In addition, in February 2023, Arkansas began reviewing cases of able-bodied, working-age adults. These individuals are perhaps the most likely to have experienced changes, such as earning higher income, that would affect their eligibility given that they are in their prime working years and many of them may have become eligible for Medicaid in the first place due to pandemic-induced job loss.
Arkansas is also resisting the ACA’s perverse funding incentive to target traditional Medicaid enrollees for redetermination. Because the federal government pays a much higher share of the costs of ACA expansion enrollees, states have a financial incentive to redetermine traditional Medicaid enrollees first.32 Doing so would save them more state dollars than removing ACA expansion enrollees would, because federal taxpayers pay much less for the traditional populations, who also tend to be more expensive.
Here are seven steps that states should take to perform expedited and efficient redeterminations.
The COVID-19 pandemic and the continuous Medicaid enrollment provisions enacted by Congress have led to a surge of Medicaid enrollment and spending. Ineligible and improperly classified Medicaid enrollees was already a massive program integrity problem prior to the pandemic because of the ACA. There are now nearly 20 million people enrolled in Medicaid who are not eligible for the program, almost all of whom have access to another source of subsidized health coverage. States have an obligation to move as quickly and smartly as possible to begin cleaning up their Medicaid rolls. Doing so would represent an important first step toward rebuilding public trust, protecting taxpayers, and preserving resources for the country’s most vulnerable.
