
Brian Blase, Ph.D.
Brian Blase, Ph.D., is the President of Paragon Health Institute. Brian was Special Assistant to the President for Economic Policy…
Reforming Government, Empowering Patients
Navigation
The paper critiques Medicaid DSH payment allocations, showing a bias against non-Medicaid expansion states, stressing the need for reform to fairly support hospitals serving low-income populations.
The House-passed Build Back Better (BBB) Act cuts federal funding to hospitals in states that have not expanded Medicaid under the terms of the Affordable Care Act (ACA), but not in states that have expanded Medicaid.1 The cuts would specifically result from a 12.5 percent reduction in Medicaid disproportionate share hospital (DSH) funding to non-expansion states.2 DSH payments are the only type of Medicaid payment in statute that is explicitly intended to cover a portion of unpaid services hospitals provide to uninsured patients.3 DSH payments also serve to somewhat offset low Medicaid rates since base Medicaid payments often do not cover the hospitals’ costs of providing services.4
DSH payments have never aligned well with the program’s aims. Federal DSH funds are inequitable distributed across states, and Medicaid expansion states generally receive much larger federal DSH funding allotments than non-expansion states. The BBB Act’s reduction of federal DSH funds to only non-expansion states would worsen this inequity.
Most payments received by hospitals are direct payments for health care (fee-for-service payments) and payments from managed care plans to providers for services delivered (Medicaid managed care). States also make payments of federal funds to hospitals and other providers that are not direct payments for the services they provide. These “supplemental” payments include DSH payments, upper payment limit (UPL) payments, uncompensated care pool (UCP) payments, and delivery system reform incentive (DSRIP) payments.5
The BBB Act cuts not only DSH funding but also federal UCP assistance to non-Medicaid expansion states (but not to expansion states) by excluding payments from the UCP made on behalf of people who would be eligible for Medicaid if the state adopted the ACA’s expansion. Eight states, including four non-Medicaid expansion states—Florida, Kansas, Tennessee, and Texas—receive UCP funding. The Congressional Budget Office projects the cuts to Medicaid’s DSH and UCP programs would reduce federal spending by a total of $18.3 billion from 2023-2026 and $34.5 billion from 2023-2031.6
As the BBB Act moves to the Senate, hospitals are unsurprisingly pushing back on the legislation’s DSH cuts.7 Several senators have been vocal about their opposition to the cuts, including both Democratic senators from Georgia,8 Raphael Warnock and Jon Ossoff, and all six Republican senators from Florida, Tennessee, and Texas.9
The House-passed legislation also contains large tax cuts for upper-income households in states with high state and local taxes, such as California and New York, through a provision which expands the amount of state and local taxes that can be deducted from income for federal tax purposes.10 The BBB Act’s cuts to DSH and UCP funding for those in need combined with huge tax cuts for the wealthiest have led Republican senators, such as Marco Rubio of Florida, to frame the issue this way:
The … bill is going to hurt Florida hospitals, especially those that treat low-income residents and the uninsured. It is reckless and irresponsible to cut the health care of some of our most vulnerable, including children, to pay for tax cuts for wealthy taxpayers in New York and California.11
In contrast, leading House Democrats suggest that the proposed DSH cuts make sense because other provisions of the BBB Act authorize subsidies for people in non-Medicaid expansion states with incomes below 100 percent of the poverty line. Under the BBB Act, these individuals—who are currently ineligible for both Medicaid and premium subsidies—would be entitled to enroll in an exchange plan with a zero out-of-pocket premium and minimal cost-sharing. Rep. Frank Pallone (D-New Jersey), chairman of the House Energy and Commerce Committee, laid out the rationale for the DSH cuts as follows:
The people that are in those red states that were in that Medicaid gap, once they access the ACA and they have insurance, that’s gonna more than make up for the hospitals and the caregivers in terms of whatever they’re getting from the state for uncompensated care.12
This paper will show that Rep. Pallone’s rationale for cutting funding to safety net hospitals just in Medicaid non-expansion states is problematic. States that have not adopted Medicaid expansion receive far less in federal assistance to finance health care services for the uninsured and low-income populations. The BBB Act would increase these inequities and harm safety net hospitals in poorer and more conservative states. Rather than the irrational approach in the BBB Act, policymakers should reform Medicaid financing and ensure that federal funds are more equitably distributed across states.
The key feature of the joint federal-state Medicaid program is an open-ended federal reimbursement of state expenditures. States with lower per capita income have a higher percentage of their Medicaid expenditures reimbursed by the federal government than wealthier states do. Under the program’s formula, the federal government reimburses half of state Medicaid expenditures in states with the highest per capita income and roughly three-quarters of expenditures by states with the lowest per capita income. The federal percentage, or share of a state’s spending, is referred to as a state’s federal medical assistance percentage (FMAP).
Despite the higher reimbursement percentages for poorer states, wealthier states have developed much more expansive Medicaid programs, largely through broader eligibility categories and benefits. In reality, the federal government provides much more financial support for lower-income individuals’ health care services in wealthy states than in poorer states. These inequities in federal funding have grown with the ACA’s Medicaid expansion because the wealthy states and those with already profligate programs were more likely to expand.
In 2018, federal Medicaid spending per person in poverty equaled $9,051.13 The correlation between state per capita income and federal Medicaid spending per person in poverty provides a proxy for whether the federal Medicaid financing provides greater support to states with lower levels of fiscal capacity. If the federal government were providing greater Medicaid funding to poorer states, this correlation would be negative.
However, wealthy states receive much greater federal Medicaid support per person in poverty than poorer states do. In fact, the correlation between federal spending per person in poverty and state per capita income (r=0.58) is high and positive.14 Wealthy states—such as New York, Massachusetts, Connecticut, New Hampshire, Vermont, Minnesota, and Maryland—receive federal funding per person in poverty well above the national average, while states with lower per capita incomes tend to receive much lower support per person in poverty. In other words, the federal government’s FMAP formula has incentivized the wealthy states to grow their Medicaid programs through broader eligibility, expanded benefits, and higher payment rates. Through these expansions, these states have successfully received much more funding from the federal government than poorer states have, despite the higher FMAP percentage for poorer states. Of note, excluding Medicaid expansion funding reduces the correlation between state per capita income and federal Medicaid spending per person in poverty, but only slightly to 0.54.15 Thus, although Medicaid expansion worsened the disparity in federal Medicaid payments between wealthier and poorer states, that disparity largely pre-dates Medicaid expansion.
In addition to the basic funding formula, the federal government also provides states with DSH funding. DSH payments are intended to compensate hospitals that provide significant amounts of uncompensated, or poorly compensated, services. The DSH program has two essential features: 1) federal dollars are distributed to states, and 2) states make payments to hospitals.
States began making Medicaid DSH payments to hospitals in 1981, but states were required to provide actual financing for their share of the payments, so DSH payments remained low.16 The federal government then reimbursed each state at its FMAP rate for the payments it made to eligible hospitals.
However, in the mid-1980s, the federal government issued a regulation and guidance that permitted states to fund their share of DSH payments with financing gimmicks, enabling the states to receive federal payments without having to actually pay their share. These gimmicks have been well-documented and effectively result in states obtaining federal Medicaid funds without having to make actual state contributions.17
One such gimmick is a Medicaid provider tax. A state raises funds from a health care provider such as a hospital or nursing home, uses that tax revenue to make Medicaid payments to those providers, obtains federal funds through its Medicaid reimbursement, and then makes those providers whole through higher payments financed entirely by the federal funds.
According to the Medicaid Access and Payment Commission (MACPAC), “This combination of unlimited DSH payments and financing flexibility was soon followed by a significant growth in DSH spending and, from 1990 to 1992, the total amount of DSH payments increased from $1.3 billion to $17.7 billion.”18 In 1992, Congress capped federal DSH funding to states due to concerns that federal DSH spending was surging unsustainably and “that some states were misusing DSH funds by making large DSH payments to hospitals operated by state or local government that were then transferred back to the state and used for other purposes.”19 This cap essentially locked states into the level of DSH they had in 1992, with only adjustments for inflation since 1992.20 As a result, states that had employed the most gimmicky financing schemes to maximize DSH by 1992 have reaped a windfall over the past three decades compared to states that had not employed such schemes.
States also have broad authority to determine the amount of DSH payments that hospitals receive. The DSH payments are supposed to be targeted to hospitals that provide greater amounts of uncompensated care, but in reality, political factors can influence states’ allocations to hospitals. For example, according to an audit by the Government Accountability Office, “states generally provided more DSH payments to public hospitals (in comparison to private and non-profit hospitals) and teaching hospitals (as compared to non-teaching hospitals) relative to their share of total uncompensated care costs.”21 In practice, states can designate almost any hospital as eligible to receive DSH payments if the hospital has a Medicaid utilization rate of at least one percent.
States’ flexibility over DSH payments to hospitals combined with the huge variation in federal DSH allocations to states have led some states to make DSH payments to nearly all their hospitals while other states provide DSH payments to only a few hospitals.22 Hospitals providing little uncompensated care in states with excessive federal DSH funding often still receive DSH payments because their states are spreading out the excessive funding, while hospitals providing much more uncompensated care in states with low federal DSH funding receive less support through the program.
The main provisions of the ACA significantly increased federal spending for health insurance through both exchange premium subsidies and Medicaid expansion. This new federal spending, which in 2020 totaled about $130 billion, reduced the number of people without coverage.23 The ACA contained large cuts to DSH—with reductions approaching 40 percent of federal DSH funding—because its spending provisions were projected to significantly reduce hospital-provided uncompensated care, which it has in fact done. One study found that uncompensated care costs declined from 4.1 percent to 3.1 percent of operating costs in 2014, the year when the Medicaid expansion took effect.24 A second study found similar results: uncompensated care costs declined by about 30 percent more in Medicaid expansion states than in non-expansion states in 2014.25
Despite the decline in uncompensated care, the powerful hospital lobby pushed back on the DSH cuts included in the ACA, and the hospitals have convinced Congress to repeatedly delay them.26 The cuts are supposed to begin again in fiscal year 2024—at an amount of $8 billion per year.
While federal Medicaid DSH payments are a small percentage of overall Medicaid funding, this program could be an efficient use of taxpayer resources by well-targeting those resources to hospitals where the need is greater. For example, the safety net financing approach may be much more efficient in non-expansion states than in expansion states. Non-expansion states can use federal funds—through DSH payments as well as other supplemental payments—to directly subsidize providers to treat uninsured people who have limited ability to finance their care as well as to make up for funding shortfalls from Medicaid.
In contrast, in expansion states that increased Medicaid eligibility to working-age, nondisabled, and generally childless adults who typically do not consume much medical care, federal funds are used to reimburse states for high expansion-related expenditures to insurers. This financing approach also produces unintended consequences that include the replacement of private coverage with public coverage and the displacement of care as some people with more pressing health needs are crowded out by those with less pressing health needs.27
Medicaid expansion has also caused a surge in improper payments in the program, which now approach $100 billion.28 These improper payments largely consist of government payments to insurers to administer managed care on behalf of enrollees who are not eligible for the program or who may not be eligible for the program (as their eligibility was not properly determined).29
Expansion states have benefitted from both the postponement of DSH payment cuts as well as the federal funds from expanding Medicaid. For the first three years of the expansion (2014-2016), the federal government paid states 100 percent of the costs of the expansion population. While that rate gradually declined starting in 2017, it is currently 90 percent and is scheduled to remain at 90 percent under current law.30
Since many expansion states also benefit from their dodgy financing schemes that maximized their DSH payments in the early 1990s, the inequities in DSH payments across states now border on the absurd. Federal DSH funding per uninsured person averaged $432 in fiscal year 2021. Eight states plus the District of Columbia (D.C.) receive federal DSH payments of more than $1,000 per uninsured: D.C.—$2,940; New Hampshire—$2,216; Louisiana—$1,965; New York—$1,883; Rhode Island—$1,775; Massachusetts—$1,749; Maine—$1,158; Connecticut—$1,127; and New Jersey—$1,088. All these states have adopted the ACA Medicaid expansion. On the other hand, five states receive federal DSH funding averaging less than $100 per uninsured person: Wyoming—$4; Utah—$75; Oklahoma—$76; Tennessee—$77, and Florida—$84.31 Overall, Medicaid expansion states receive an average of $674 in DSH funds per uninsured, more than two-and-a-half times the $249 in DSH funds per uninsured that non-expansion states receive.32
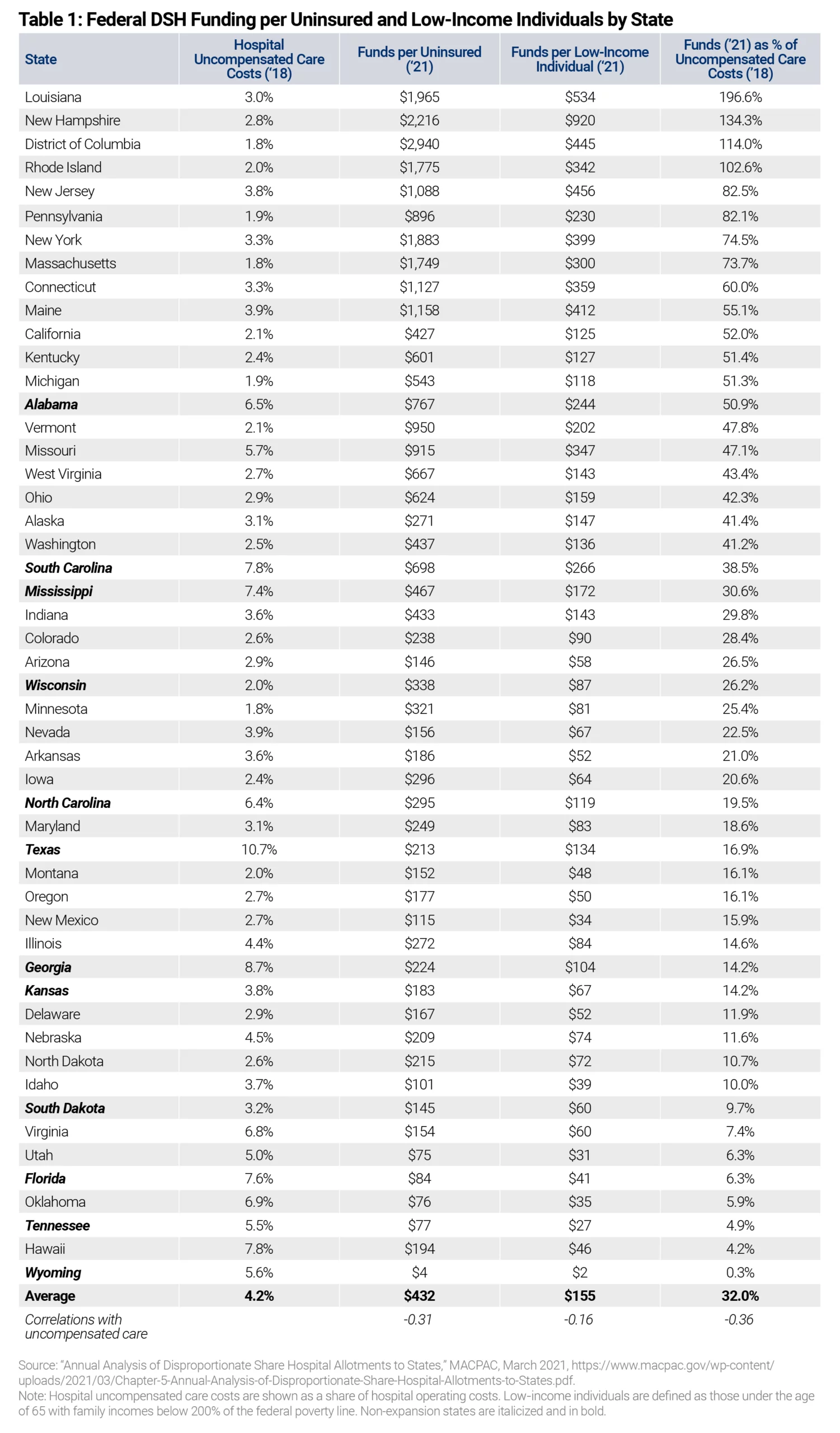
Federal DSH funds are also inequitably distributed based on a state’s low-income population (defined by a person who lives in a household with income below 200 percent of the federal poverty level). The national average of DSH funds per low-income individual is $155.33 Eight states, as well as D.C., receive federal DSH payments that are more than twice the national average: New Hampshire—$920; Louisiana—$534; New Jersey—$456; D.C. —$445; Maine—$412; New York—$399; Connecticut—$359; Missouri—$347; and Rhode Island—$342. All these states are Medicaid expansion states. Ten states receive DSH funding per low-income individual that is less than one-third of the national average: Wyoming—$2; Tennessee—$27; Utah—$31; New Mexico—$34; Oklahoma—$35; Idaho—$39; Florida—$41; Hawaii—$46; Montana—$48; and Oregon—$50. Overall, Medicaid expansion states receive an average of $182 in DSH funds per low-income individual, which is nearly 70 percent more than the average $110 in DSH funds per low-income individual that non-expansion states receive.34
Perhaps the best way to demonstrate the inequity of DSH funds is to contrast federal DSH funding as a percentage of uncompensated care provided by hospitals in each state. Overall, federal DSH funds covered an average of 48 percent of uncompensated care in Medicaid expansion states versus 17 percent of uncompensated care in non-expansion states.35 In three states (Louisiana, New Hampshire, and Rhode Island) plus the District of Columbia, federal DSH funds actually exceed the amount of uncompensated care provided by hospitals.36 In another five states (New Jersey, Pennsylvania, New York, Massachusetts, and Connecticut), federal DSH funds exceed 60 percent of uncompensated care. The top 13 states, including D.C., are all Medicaid expansion states. On the other side of the distribution, federal DSH payments cover less than 10 percent of uncompensated care in nine states (Wyoming, Hawaii, Tennessee, Oklahoma, Utah, Florida, Virginia, South Dakota, and Idaho), and another dozen states receive federal DSH payments that only cover between 10 percent and 20 percent of their uncompensated care costs.
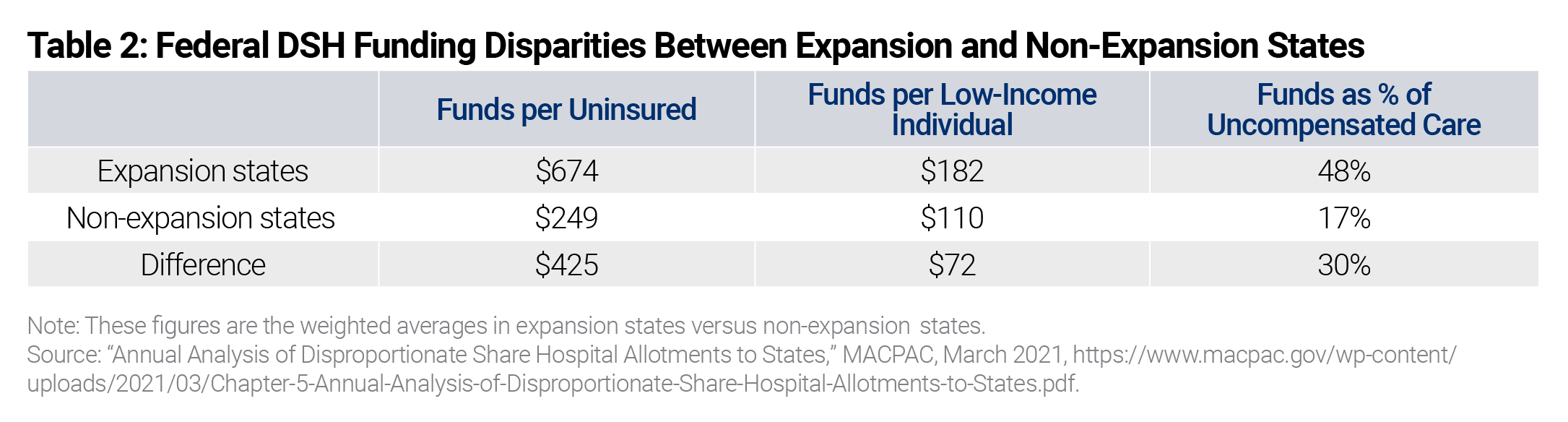
Table 2 summarizes the differences in DSH funding between Medicaid expansion and non-expansion states, showing the large disparities in funding. Of note, the correlations between the percentage of uncompensated care provided by state hospitals and federal DSH funding per uninsured (r=-0.31) and federal DSH funding per low-income individual (r=-0.16) are both negative. This means that less federal DSH funding is going to states with higher rates of uncompensated care, further evidence that the allocations across states are illogical.
The 12 states that have decided not to expand Medicaid, including Florida, Georgia, Tennessee, and Texas, have kept their programs focused on more vulnerable populations, such as low-income pregnant women, children, seniors, and people with disabilities. Their decisions have been justified. Wait times for appointments,37 ambulance response times,38 and unnecessary visits to emergency rooms39 have all significantly increased in Medicaid expansion states, indicating that resources have been redirected away from people who most need care. Medicaid expansion has not been associated with overall improvements in health outcomes.40 In fact, states that expanded Medicaid had worse mortality trends than states that did not expand Medicaid from 2014-2017, the first four years of the expansion.41
In addition to the disappointing health outcomes, the fiscal cost has been massive. Taxpayer spending exploded in expansion states, with enrollment busting past projections and improper payments soaring to unprecedented levels. The ACA’s Medicaid expansion drove a quadrupling of federal improper payments in the program,42 which now equal about $100 billion annually.43 In addition, other problems with the expansion include the crowding out of other public priorities, the replacement of private coverage with public coverage, and increased financial dependency of state governments on a federal government with a monstrous national debt and expanding annual deficits.44
For 30 years, the DSH formula has harmed states that had not by 1992 utilized creative financing gimmicks to maximize federal payments. In general, the states that adopted the ACA’s Medicaid expansion were also the ones that have unfairly benefitted from Washington’s decision to lock state DSH funding allocations into place for the past three decades.
Cutting DSH payments to non-expansion states while retaining them for expansion states—as the BBB Act would do—only increases this inequity, further harming those whom Medicaid was originally designed to assist. Cutting DSH just in non-expansion states seems particularly unfair because those states have saved the federal government hundreds of billion dollars over the past eight years by not expanding Medicaid, thereby not adding to the country’s growing federal debt.
Leading congressional Democrats point to the BBB Act’s temporary premium subsidies, which are designed to assist people with income below the poverty line to obtain health coverage, as the rationale for the proposed DSH cuts in only non-Medicaid expansion states. It is also true that congressional Democrats are frustrated by the decisions of non-expansion states to turn down the ACA’s terms.45 In early 2021, congressional Democrats further enticed holdout states to expand by including enhanced payments in the American Rescue Plan Act for states that newly adopt the expansion. This attempt failed to convince any holdout states to expand. Cutting DSH and UCP funding only in non-expansion states is another attempt to coerce states into expanding their Medicaid programs. The carrots have not worked, so Congress is now using the stick.
The purported rationale from congressional Democrats, which ignores the underlying inequities in DSH funding, falls apart for two additional reasons. First, the premium subsidy expansion would last only through 2025, but the DSH cuts would be permanent in non-expansion states. Second, if Congress wishes to cut DSH because other government subsidies have reduced uncompensated care, the DSH cuts should apply both in expansion states, where lower-income people are eligible for Medicaid per the ACA, and in non-expansion states, where lower-income people would be newly eligible for heavily subsidized exchange plans. In fact, many of the exchange plans are essentially Medicaid managed care plans.
Federal financing of Medicaid needs significant reform. The main reason for needed reform—federal Medicaid spending is approaching $500 billion annually46 without generating sufficiently beneficial outcomes. Instead, the health of lower-income populations continues to deteriorate, medical resources are being misdirected, improper spending exceeds one-fifth of program expenditures, and exploding Medicaid growth is crowding out other vital public priorities. Fundamental and meaningful Medicaid financing reform would realign states’ incentives, away from using Medicaid to maximize federal payments and instead toward obtaining the best outcomes and value for program recipients and taxpayers supporting the program.
In the absence of large-scale reforms, there are many smaller, more targeted reforms that could further these aims. One such reform would be to DSH—to disburse funds more equitably across states and to better target those funds to safety net providers within states. In fact, Congress could consider merging all of Medicaid’s supplemental programs into one program with a more rational allocation across states.
DSH reforms are needed because the federal government locked states into the same payment rates for the last three decades based on states’ use of creative financing schemes at the time. This has resulted in large and unfair transfers across the states and the irrational allocation of federal support for safety net hospitals. As a result of the ACA’s Medicaid expansion, the disparities in federal funding for uninsured and lower-income populations became more absurd. The result: Medicaid DSH transfers money from states such as Tennessee, Florida, Kansas, Georgia, and Texas (non-expansion states that did not employ gimmicky schemes to maximize federal DSH funds) to states such as New Hampshire, Louisiana, New York, Massachusetts, Connecticut, and New Jersey (expansion states that did employ gimmicky schemes to maximize DSH funds). These transfers have no policy rationale or justification. If policymakers want to sensibly reduce federal DSH payments, they should make the cuts primarily to expansion states.
Federal DSH funding, and Medicaid supplemental payments in general, should be allocated amongst states based on the amount of uncompensated care provided by hospitals in those states. Since it is politically difficult to change funding allocations across states immediately, there could be a multi-year transition to move from the inequitable status quo to a fairer state allocation. Federal rules should also be tightened to ensure that states distribute the funds to the hospitals with the most need—hospitals that treat the greatest number of uninsured and low-income patients—instead of hospitals with the most political clout.