
Theo Merkel
Theo Merkel is the Director of the Private Health Reform Initiative and a Senior Research Fellow for the Paragon Health…
Reforming Government, Empowering Patients
Navigation

This paper discusses the shift towards price transparency in U.S. healthcare, highlighting improved pricing clarity for consumers and recommending further policy enhancements for better compliance and accessibility.
Pricing information, and with it the ability to compare relative prices of alternatives, is an extremely important part of how both consumers and suppliers discern value for most items and services in the United States. Yet decades of laws and regulations eroded the incentive for prices to be disclosed in health care—even for routine, non-emergent, and shoppable care.
The Trump administration dramatically changed that status quo with two major regulations that force health care providers and payers to disclose actual prices to the individual patient and comprehensive pricing data to the general public. Congress followed suit by requiring providers and payers to provide personalized pricing information to patients in advance of care.
Reversing decades of opaque pricing has not happened overnight, but there have been positive developments along the way to full implementation of the three major federal price transparency provisions. This report provides a brief overview of recent federal action, suggests reasons for optimism despite slow and uneven compliance, and makes six recommendations to policymakers for improvement:
When President Trump signed the health care price transparency executive order in the Entrance Hall of the White House on June 24, 2019, supporters knew that uncovering clear and straightforward prices for medical care still faced an uphill battle. The intervening four years have witnessed the resolution of the major legal challenges, continuity between administrations, the initial phase of implementation and utilization, and a groundswell of bipartisan support.
As a former White House official who helped develop and design the price transparency regulations in the Trump administration,1 this author sees these early results as encouraging. Stakeholders have pointed out meaningful improvements to make the reported prices more accessible and easier to use, but policymakers should be wary of broad changes that could upheave progress before the foundations have settled.
This report provides an overview of recent federal action on health care price transparency, suggests reasons for optimism despite slow and uneven compliance, and makes recommendations for improvement.
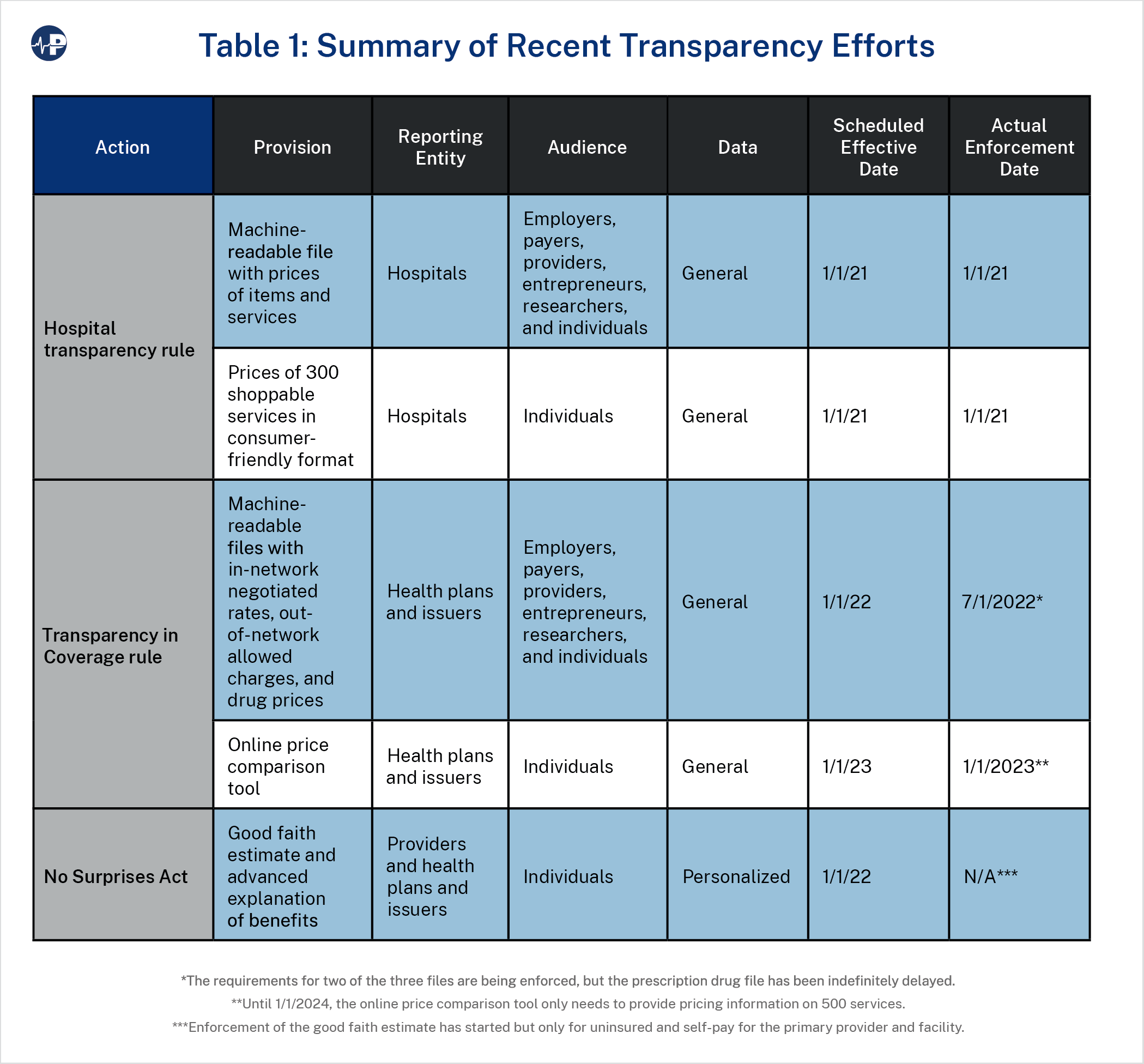
Federal action on health care price transparency has had three main thrusts. The first two originated from requirements in the Patient Protection and Affordable Care Act (P.L. 111-148 and P.L. 111-152)—first fully executed by the Trump administration (Executive Order 13877) and then strengthened by the Biden administration (Executive Order 14036). Congress passed the third in the No Surprises Act at the end of 2020.2
Hospital Transparency3
Beginning January 1, 2021, hospitals were required to make public a comprehensive machine-readable file with the prices of all items and services provided by the hospital, including the negotiated rates with payers (including commercial insurers, Medicare Advantage plans, and Medicaid managed care plans) and the discounted cash price. The machine-readable condition is important to ensure that these files, which were anticipated to be large, could be captured and digested with the help of technology.
Additionally, hospitals must display in a consumer-friendly format the prices for 300 shoppable service bundles, including 70 shoppable services specified by the Centers for Medicare and Medicaid Services (CMS).
The American Hospital Association sued to prevent this information from being made public. A D.C. District Court judge rejected this challenge,4 and that ruling was upheld upon appeal.5
Transparency in Coverage6
Starting on January 1, 2022, health plans and issuers in the individual and group markets were required to make public two machine-readable files. One file must include the negotiated rates with in-network providers for all covered items and services (the “in-network file”). The other must provide the allowed amounts that these payers have reimbursed out-of-network providers for items and services within a specified 90 day time period (the “allowed amount file”). These datasets cover more items and services than the hospital rule did because they include all providers that have contracts with or have received payment from payers rather than only hospitals.
The Trump administration also required a third file including the prices of all covered prescription drugs (the “prescription drug file”). Post-sale discounts and rebates between the various intermediaries in the pharmaceutical supply chain can make it difficult to know what is really being paid. Thus, the rule would have required that the machine-readable drug file include a historical net price that reflects the amount the health plan or issuer ultimately paid for the drug net of all the post-sale discounts and rebates.
Additionally, starting on January 1, 2023, health plans and issuers were to make available a consumer-facing online price comparison tool with required outputs such as the gross charge, negotiated rate, and out-of-pocket share for 500 services, with all services required to be available by 2024.
The U.S. Chamber of Commerce, its affiliate the Tyler Area Chamber of Commerce,7 and the Pharmaceutical Care Management Association (PCMA) challenged the Transparency in Coverage rule in federal court.8 The PCMA is the trade association for pharmaceutical benefit managers—intermediaries contracted out by health plans and issuers to negotiate lower prices from pharmaceutical companies—and particularly objected to disclosure of the historical net price of drugs.
Shortly after the lawsuits were filed, the Biden administration delayed enforcement of the machine-readable files by six months until July 1, 2022.9 After this move, the U.S. Chamber of Commerce and its affiliate dropped their lawsuits. In a demonstration of the support for health care price transparency among employers, the Tyler Area Chamber of Commerce, representing businesses in the northeastern Texas city of Tyler (approximately 100,000 residents), indicated it wanted to withdraw from the lawsuit “based upon feedback from community leadership.”10
In the same announcement that delayed enforcement, the Biden administration also decided to pause the prescription drug file requirement before the effective date and solicited comment as to its interaction with new requirements included in the Consolidated Appropriations Act that similar drug pricing information be reported to the Department of Health and Human Services (HHS) as opposed to being made public. This action caused the PCMA to eventually drop its lawsuit against the rule,11 but it has resulted in a subsequent lawsuit by the Foundation for Government Accountability (FGA) over failing to follow through with the full rule.12
No Surprises Act
Starting on January 1, 2022, providers and facilities were to provide a “good faith estimate” of expected charges upon the scheduling of an item or service or at request to the individual or to his or her plan, issuer, or carrier. Upon receiving the good faith estimate, the plan, issuer, or carrier was to send the covered individual an “advanced explanation of benefits” in clear, understandable language within a specified period.
However, in the same announcement that delayed the enforcement of the in-network and allowed amount machine-readable files and paused the prescription drug file indefinitely, the Biden administration indicated that it would not enforce the good faith estimate (except for uninsured or self-pay patients) or the advanced explanation of benefits until a future rulemaking establishes standards for transferring data between providers and facilities and plans and issuers. In September 2022, the Departments of HHS, Treasury, and Labor put out a request for information on the subject, but the rulemaking is still forthcoming. Implementation appears to be delayed because of concerns over the ability of providers and plans to transfer data in a standard application programming interface and safeguard personal health information.13
For uninsured or self-pay patients, enforcement of the good faith estimate requirement began on January 1, 2023, but only for the primary provider and facility. (Enforcement discretion continues for co-providers and co-facilities until the conclusion of the forthcoming rulemaking on data sharing.14)
Interaction
The fragmented nature of health care led Congress to apply transparency requirements to multiple actors when it passed the Affordable Care Act. The Trump administration sought to ensure that basic information would be available in a straightforward, accessible form for individuals (thus the 300 shoppable services in consumer-friendly format requirement for hospitals and the online price comparison tool requirement for payers) and in more comprehensive forms for employers, payers, providers, entrepreneurs, and researchers (thus the machine-readable file requirements for both hospitals and payers).
The machine-readable files, while in their initial form only digestible to more sophisticated data experts, provide potentially the broadest and most transformative value. Implemented properly, these will provide the robust data sets needed for employers to identify better value, payers to negotiate better contracts, more efficient providers to undercut competition, developers to engineer travel app-like tools for individual patients and consumers, and applications not yet imagined.15
After the regulatory actions, Congress determined that in addition to the general information already required to be made public, potential patients should be able to get more personalized information on network status and expected charges in anticipation of care (thus the good faith estimate and advanced explanation of benefits).
Much of the commentary around the implementation of health care price transparency has been around the size, complexity, and sometimes poor quality of the machine-readable files. What has gotten less attention is that even while the kinks are being worked out, newly available pricing data is being utilized in a way that is helping patients get better value.
A straightforward example comes from one of the consumer-facing provisions. A Wisconsin woman highlighted by CMS in Health Affairs16 saved $1,000 on two tests by going to a different location of the same hospital system just 20 minutes away. Using the hospital’s publicly posted shoppable services, the patient found a CT scan for 60 percent less than the one she was originally scheduled for and an echocardiogram for 45 percent less.17 She then verified that lower cost was what she was actually charged—complete with a screenshot of her explanation of benefits. This example is a vivid demonstration of savings that patients, albeit well-informed and well-motivated ones, are achieving with their newfound access to prices—in this situation without even leaving the same hospital system.
The machine-readable files themselves, while not yet meeting their full potential, are still being used in productive ways. In conversations with those on the forefront of price transparency efforts, Paragon has heard from a major consulting firm helping lower-cost providers make the case to payers to drive more patient volume in their direction. Entrepreneurs have relayed how they are providing pricing data to employers to compare rates to those of other payers and to other providers in the same region.
In December 2022, multiple unions utilized pricing information from the publicly available machine-readable files as part of a lawsuit against Elevance, the insurance company formerly known as Anthem, alleging that the charges billed for were higher than those agreed to in their contract.18 An employer-led health care coalition, the Employers’ Forum of Indiana, has enhanced its public-facing hospital transparency tool by using data from the hospital machine-readable files, aggregated and cleaned by the transparency-focused start-up Turquoise Health.19 Researchers have used the data to reinforce concerns over dramatic variation in health care services among regions, within a region, even within a single hospital, and how cash prices are often lower than even the lowest negotiated rate.20
Despite the initial implementation, the average patient, employer, or other interested party does not yet have easy access to clear prices for any health care service or item of his or her choosing. Significant improvements should happen for several reasons: Compliance is improving, data experts and entrepreneurs are learning how to manage and translate the massive amounts of data, and stakeholders are becoming more familiar with the opportunities that health care price transparency presents.
Compliance Is Improving
As mentioned above, the hospital rule was the first transparency provision to take effect. Patient Rights Advocate, a nonprofit organization focused on promoting system-wide health care price transparency, and others have well documented that initial compliance was dismal. In July 2021, Patient Rights Advocate found only 5.6 percent of the random 500 hospitals they surveyed in compliance with the rule.21 Low initial compliance likely results from a variety of factors, including COVID-19, uncertainty over litigation, and the initial very modest civil monetary penalty for non-compliance of $300 per day.
Encouragingly, the Biden administration increased the penalty to a scale based on number of hospital beds at a facility with a new maximum fine of $5,500 per day (over $2 million per year) starting on January 1, 2022. While CMS has been reluctant to enforce the penalty so far, in April 2023 the agency reported sending out 730 warning notices and 269 requests for corrective action plans.22 As displayed in Figure 1, these moves have led to a corresponding increase in the number of hospitals posting machine-readable files.
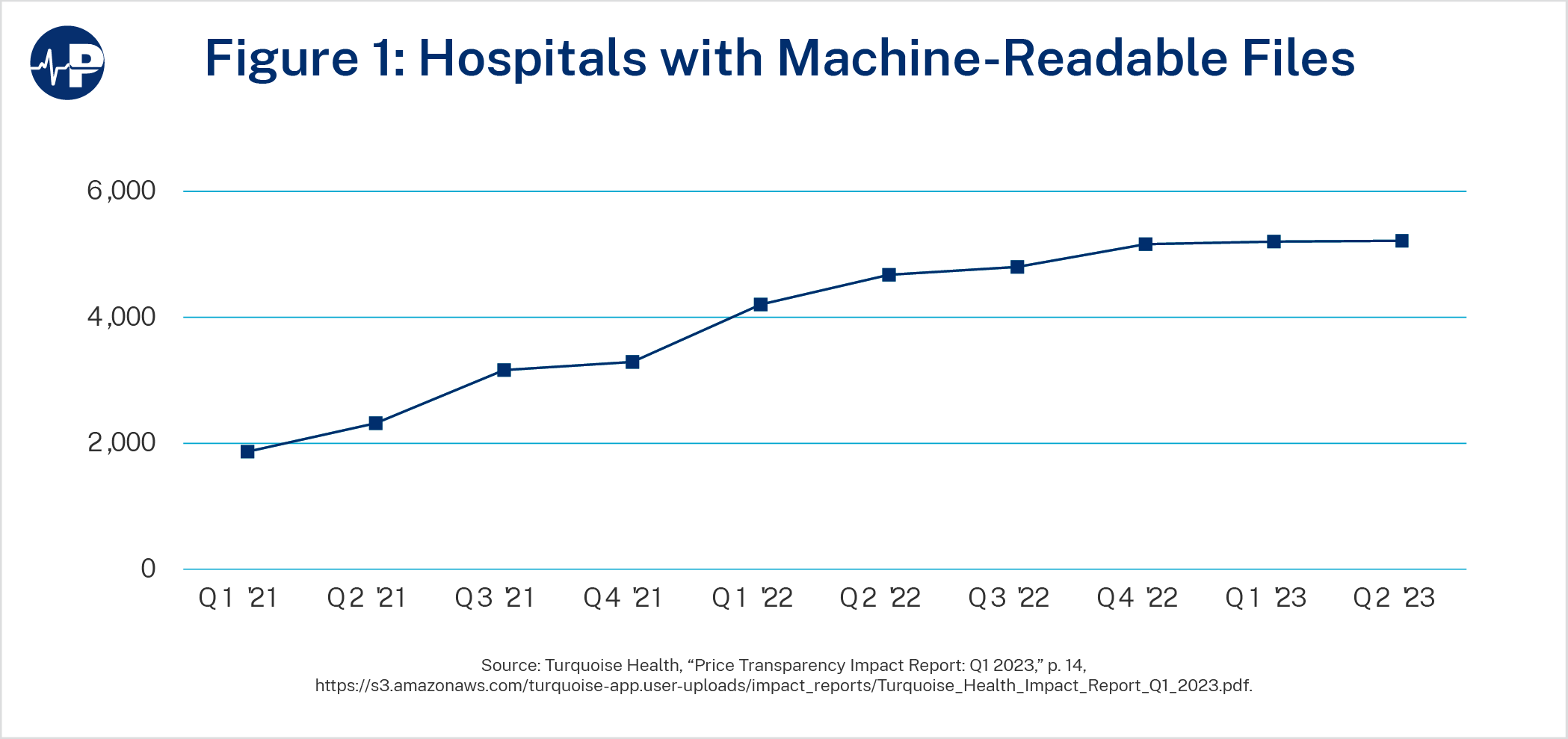
Just posting a file is the bare minimum and says nothing about quality or accuracy, but the trend shows clear progress. This is despite significant accommodations made by CMS to those in violation of the regulation, as the FGA illustrated in a recent report.23
Compliance with the Transparency in Coverage rule by health plans and issuers has been both better and worse than hospitals’ compliance. The percentage of payers that have publicly displayed machine-readable files within the first six months is higher than that of hospitals.24 However, there are still concerns over quality and potentially the accuracy of the data—reinforced by variation in the prices being reported from month to month.25 The Transparency in Coverage rule did go into effect a year and a half after the hospital rule, and there has also been limited public notice of enforcement actions by either the federal government or states—the primary enforcers of the applicable section of the Public Health Service Act.
Data Experts and Entrepreneurs Are Catching Up to Complexity
Starting in January, Health Affairs Forefront ran a series of posts on price transparency,26 including observations on the data itself and the resulting research, recommendations for improvements,27 and instructions for those seeking to use the information for app development.28 This provides a snapshot of what has been published in the larger health literature since the rules took effect. Even more exciting is the stream of activity in the health sector, from legacy consulting firms to a range of start-ups using various approaches to transform the health pricing data into actionable information. Not all approaches will succeed, but the public availability of the pricing data should allow the best methods to rise to the top.
Stakeholders Are Becoming Increasingly Aware of Opportunities
As Brian Blase has pointed out, employers are particularly well positioned to take advantage of price transparency in health care.29 Employers have strong incentives to lower health care spending to attract employees with higher wages. Employers may have more flexibility than insurers do, as insurers typically desire to maintain relationships with local providers, and hold more leverage from volume and larger financial resources at stake than the individual consumer. However, all but the most aggressive human resources departments tend to be risk-averse and reluctant to innovate, as health care is usually not the source of the business’ marginal advantage and is primarily provided as a benefit to attract and retain employees. To the extent that human resources departments stay inactive in this fight, they are leaving a significant opportunity on the table to increase savings, maximize the overall compensation provided to their employees, and attract the best possible workforce.
In September 2022, the National Alliance of Healthcare Purchaser Coalitions, a nonprofit that represents over 12,000 employers covering 45 million Americans, released a public playbook on how employers can use health care price transparency to obtain more value for their employees.30 Patient Rights Advocate has published case studies of employers and labor unions using transparency to lower health care costs for their employees and members.31 As industry leaders and advocacy organizations demonstrate success and provide best practices, more employers will likely use price transparency to improve the value of their health benefits.
The health care price transparency rules sought to make information public quickly and in a decentralized way. This was by design and an acknowledgement that the federal government does not have a monopoly on the best ideas for how to display prices. While this has made implementation unusually public (and at times, described as “messy”), it has allowed supporters and critics alike to provide constructive feedback on how to improve the process. There are several steps the Biden administration, Congress, and states could take to improve the effectiveness of the rules and expand health care price transparency.
Congress should codify the general framework of the transparency regulations, with special attention to the most comprehensive elements—the public disclosure of negotiated rates for both hospitals and payers in a machine-readable format. This should provide additional assurance to stakeholders that it is worth investing in solutions based on price transparency and dissuade further effort from opponents to undermine the rule or not comply.
The House of Representatives, where jurisdiction over these policies is shared by three committees, has started to move bipartisan legislation to do just this. On May 24, the Energy and Commerce Committee reported out the Promoting Access to Treatments and Increasing Extremely Needed Transparency (PATIENT) Act, which includes language to codify the hospital and health plan transparency regulations, with minor modifications, by a unanimous vote of 49-0. On July 12, the Education and Workforce Committee passed a similar codification of the provisions within its jurisdiction, the Transparency in Coverage Act, by a vote of 38-1.
On July 26, the Ways and Means Committee reported the Health Care Price Transparency Act to codify the transparency rules by a vote of 25-16, with those voting against it largely expressing concerns about subject matter unrelated to the overwhelmingly bipartisan price transparency provisions.32 The Ways and Means Committee would take positive steps to put many transparency requirements into statute, but it partially undermines the purpose of codification of the hospital rule by granting the secretary of HHS discretion over whether to require disclosure of payer-specific negotiated rates. The previous secretary of HHS has discretion under current law and determined that the best interpretation of standard charges (the term used in current statute) is the actual price paid for items and services—the payer-specific negotiated rate. Explicitly saying a future secretary can reverse this progress is misguided and could empower the opponents of broad price disclosure.
The enhanced discretion appears to be out of concern for overlap between some of the content in the prices disclosed by hospitals and payers. When evaluating this concern, policymakers should keep in mind that price disclosure by providers should be the natural state of affairs, as it is in other industries, and the current opacity has only been enabled by other misguided policies.33 Hospitals have also already begun to disclose these prices. Therefore, additional compliance cost should be minimal. Finally, hospital disclosure of payer-specific negotiated rates provides value distinct from the value of the Transparency in Coverage rules as the format is more easily searchable for consumers and employers, and it includes more payers. (Notably, hospitals disclose the prices they charge Medicare Advantage and Medicaid Managed Care plans.)34
States frustrated with lack of compliance with the hospital price transparency rules have also moved to codify the requirements into state law, often with additional penalties. Thus far, Arizona,35 Colorado,36 Minnesota,37 Texas,38 and Virginia39 have all successfully passed measures. Legislation has been introduced in approximately 20 states.
The threat of enforcement action has improved the amount of data that is being reported, but the usability of both the hospital and health plan data continues to suffer from lack of compliance. The Biden administration made a significant and productive step in strengthening the civil monetary penalty for non-compliance of the hospital rule, and it should now assess that enhanced penalty on facilities that still refuse to appropriately report. In a recently proposed rule, CMS has also suggested that it may require hospitals to attest to the accuracy of the pricing data presented, another positive step. Congress should codify the enhanced penalty and attestation for hospitals in statute. The PATIENT Act as unanimously reported out of the Energy and Commerce Committee would put the enhanced penalty into statute. The Ways and Means Committee–reported language takes the enhanced penalty a step further by creating an additional penalty for persistent noncompliance.
For the Transparency in Coverage rule, the size of the penalty has never been a problem. Health plans and issuers out of compliance with the applicable section of the Public Health Service Act could face a maximum penalty of $100 per day per member. However, as is the case with other federal health insurance regulations, the final rule explains how enforcement is shared by the states and the federal government:
[S]tates will generally be the primary enforcers of the requirements imposed upon health insurance issuers by the final rules. The Departments expect to work closely with state regulators to design effective processes and partnerships for enforcing the final rules
While states may have initially been tepid to embrace their role in enforcing price transparency due to lack of experience with the new requirements, the popularity of making health care prices transparent and strong bipartisan support provides an opportunity for states to bolster their reputation on health care issues. Already, several state legislatures have introduced or passed new bills to claim power to oversee the hospital transparency requirements that were originally purely federal in nature. State enforcement of Transparency in Coverage, on the other hand, would be simply using authority already exercised by state insurance regulators. Even just one or two states that enhance enforcement could go a long way to changing the national price transparency landscape given the national reach of multiple insurers.
Senators Mike Braun (R-IN) and Maggie Hassan (D-NH) have joined to call for more aggressive enforcement for both the hospital40 and health plan transparency rules41 by the Biden administration.
When the Trump administration promulgated the transparency rules, it was working within the statutory authority Congress provided. Among providers, this authority was limited to hospitals. Congress has since revisited this with the good faith estimate requirement in the No Surprises Act, but this is limited to specific estimates for specific procedures for specific patients.
As positive steps, the Energy and Commerce Committee would institute price transparency requirements for clinical labs, and the Ways and Means Committee would add both labs and imaging.
Congress should also consider applying price transparency to ambulatory surgical centers (ASCs). ASCs are often more cost-efficient alternatives to hospital outpatient departments, and physician-owned ASCs have a strong incentive to demonstrate their relative value by publishing their prices. In fact, entrepreneurial ASCs provide some of the better examples of the positive effect of price transparency.42 However, ASCs are increasingly owned or partially owned by hospital systems.43 Applying similar price transparency requirements would thus be a way to enhance competition and the ability for patients to shop effectively for care.
The Ways and Means Committee legislation does include ASCs, though it potentially mutes the impact by giving the secretary of HHS discretion on whether to require the disclosure of payer-specific negotiated rates.
States have also begun to expand scope. When Minnesota enacted legislation to codify hospital price transparency, it also expanded the requirements to outpatient surgical centers and any medical or dental practice that has a revenue above $50 million per year.44
When implementing the Transparency in Coverage machine-readable file, the three departments that oversee the rule took proactive steps to help the public deal with the size and complexity of the files. This includes specifying a data format (json), providing a schema that standardizes what data is to be presented and how, and setting up a GitHub website with downloadable information that also serves as a venue for discussion between those interacting with the data and experts from CMS.45 The departments, and CMS in particular, should be applauded for this proactive approach.
That said, even if the original schema was perfect for that moment in time, it will need to evolve along with innovations in provider payment. While there may be some incentive for payers and providers to obscure true prices through complex contract arrangements, collaboration among industry, data and policy experts, consumers and employers, and government regulators can help ensure that the data best reflects the prices consumers ultimately pay for a service.
The hospital transparency rule includes fewer required specifications than Transparency in Coverage on how to display pricing data in the machine-readable files, which has frustrated some transparency advocates.46 Informed by recommendations from a technical expert panel, CMS recently proposed mandating the use of a template that was previously voluntary for hospitals.
As suggested by others,47 the administration (and if necessary, Congress) should ensure that consultation with a similar technical expert panel is part of a routinized mechanism to update the schema, labeling, and other relevant parameters required under both the Transparency in Coverage rule and the hospital transparency rule.
One almost universal observation on the initial implementation of the Transparency in Coverage rule has been the sheer size of the machine-readable files. Much of this was anticipated, although there are some aspects that were not. One instance has been the publishing of prices for providers that do not actually provide that service (what some have termed “zombie rates”48 or “ghost codes”50
One tension in the allowed amount file in the final rule was the balance between providing information on prices for out-of-network providers and protecting personal health information (the fear being that publishing one or two historical payments could be traced back to a specific individual). The rule therefore specified that allowed amounts for out-of-network were not to be reported unless there were at least 20 unique claims. The relatively few out-of-network providers that meet this threshold has resulted in the allowed amount file providing little value.51 As a way to ease compliance burden, Congress could consider modifying, further limiting, or ending the requirement for the machine-readable allowed amount file.
While almost all policy changes suffer from a lag time between enactment and results, federal requirements for price transparency in health care have had to contend with delays related to a global pandemic, major litigation, a change in administration, and an industry largely reticent to comply. As such, any proposed changes to price transparency requirements should be balanced against the time it may take the federal agencies to revise their regulations, stakeholders to adjust, and compliance regimes to adapt. While incremental improvements such as those suggested above would improve the initial rules, major changes to the fundamental framework of the current reporting requirements or ones that significantly increase the cost of compliance should be avoided.
Public policy experts have long claimed that health care is “different” from almost every aspect of the American economy, immune to the normal feedback loop where the value of goods and services is established by numerous, repeated, and ongoing voluntary transactions by consumers and suppliers. Over decades, some of the same experts have successfully advocated for policies—namely third-party payment, high barriers to entry, and robust government subsidization—that reinforced the same outcome they predicted. The result has been a U.S. health care system almost engineered to be opaque and inefficient. Individual patients and employers are expected to defer to insurance companies or the government to determine value for even routine care, and providers are largely insulated from more efficient competition and unmotivated to be transparent about the cost or quality of care.
As health care costs have grown as a portion of the economy and a share of the average family’s budget, the status quo has grown more and more untenable. The seemingly overwhelming preference of the “experts” has been to grant even more authority to themselves. Wage and price controls fell out of favor for most sectors of the economy back in the 1970s,52 yet they are omnipresent in health care and are routinely pointed to as a “new” solution to our ills. In September 2022, the Congressional Budget Office embraced “regulating prices paid to providers” as the most effective way to reduce health care spending for the 180 million Americans still in the commercial market53—despite the fact that federal health programs (the same programs that doom the country’s long-term fiscal solvency) have used this purported solution for over 40 years.54
The confidence displayed in price controls is breathtaking—and misplaced. Not only does it require appropriately pricing hundreds of thousands of goods and services; it also defers to government bureaucrats and politicians to shape the delivery of care, steer investment, and anticipate the health needs of tomorrow.
Price transparency is an important piece of an alternative vision. Instead of consolidating more decision-making power in the technocrat class, patients and employers should be enabled to explore their options with providers and payers competing to provide the highest value. Where patients have had both the incentive and pricing information to shop for care, the result has been cost savings55—but prior to the widespread availability of pricing information, those instances have been too infrequent.
While skeptics raise concern over the lack of incentive insured patients have to shop and the power of providers in consolidated markets, those are reasons to adopt additional reforms to empower patients and reduce barriers to entry56—not reasons why prices should be denied to patients who want them. The recent actions by the federal government, and some states, to force health care prices to be made public are about enabling more Americans to achieve the positive results seen thus far across a wider array of services. Policymakers should build off these efforts, but first they must see the new health price transparency rules through.