


Medicare currently pays providers differently for an identical service to an identical patient based simply on the building it takes place in. Policymakers have taken some steps to change this, but more can be done. Enacting “site-neutral” policies across health care settings can save taxpayers and patients money without sacrificing quality and can fight provider consolidation.
Key Takeaways
- Medicare overpays for certain services provided in hospitals that can be safely and effectively performed in a physician’s office—simply because of the site of care rather than the underlying cost. This distorts the overall health care market, including by incentivizing hospital acquisition of physician practices.
- Reimbursing based on clinical complexity or patient health status can reduce overspending by government and the private sector while reducing out-of-pocket costs for patients.
- Congress should enact site-neutral payment policies in Medicare by consolidating existing payments systems, adjusting rates, or removing other restrictions in ambulatory and post-acute care settings.
Background
Medicare’s Payment Systems
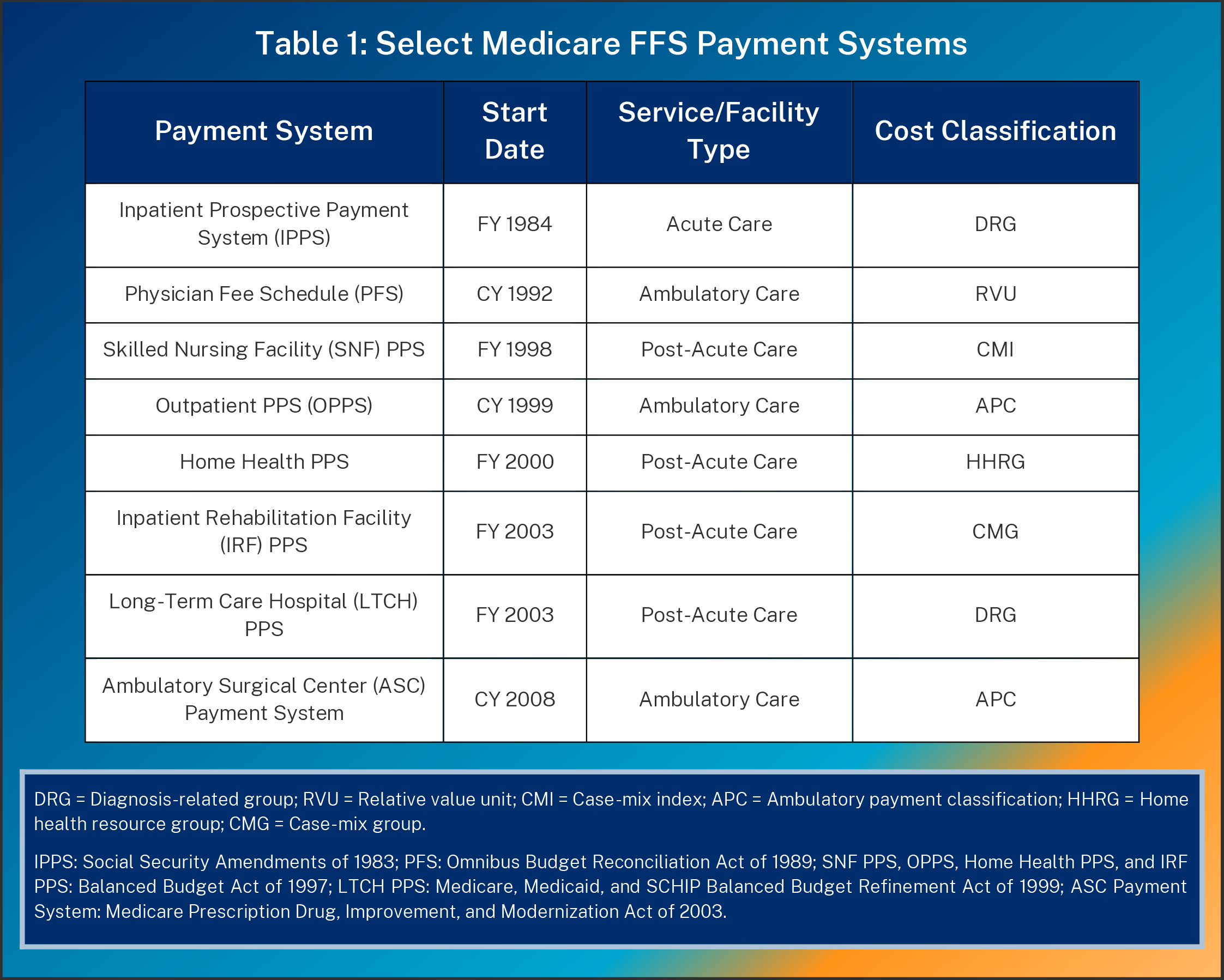
Medicare contains numerous “prospective” payment systems by provider type, with reimbursement attempting to reflect the estimated cost of providing services. The Centers for Medicare and Medicaid Services (CMS) sets a base payment rate for each payment system (sometimes called a “conversion factor”) and adjusts it by geography (e.g., local labor costs) and the service itself.
CMS calculates a service’s relative value from factors such as clinical severity or resource intensity, with different classifications in each payment system (see Table 1). This complexity can make comparisons difficult. For example, inpatient hospital services use diagnosis-related groups (DRGs) but hospital outpatient departments (HOPDs) use ambulatory payment classifications (APCs). CMS typically updates rates in annual notice-and-comment rulemaking.
HOPDs, ambulatory surgical centers (ASCs), and physicians’ offices are “ambulatory” settings where doctors perform lower-acuity services that do not require inpatient hospital stays. (In a literal sense, the patient is ambulatory, or able to walk out of the facility after receiving care.) Skilled nursing facilities (SNFs), home health agencies (HHAs), inpatient rehabilitation facilities (IRFs), and long-term care hospitals (LTCHs) provide “post-acute care” (PAC) after hospital admission.
These discrete categories suggest different types of services or patient populations, but there is often overlap. Within the ambulatory care category, doctors can perform minor surgeries in both HOPDs and ASCs or clinic visits in both HOPDs and physicians’ offices. Yet each setting has its own rules: HOPDs, for example, must have a nurse on call 24/7, while an ASC needs only a transfer plan with a nearby hospital. Since ASCs have lower regulatory costs, their payments average 60 percent of HOPDs’ (see Figure 1).1
Services provided in hospitals and inpatient settings tend to be more expensive than those provided in ambulatory settings. However, medical advances allow procedures that previously required inpatient admission to be performed as well in ambulatory settings, although Medicare regulations sometimes restrict such innovations. For example, CMS once forbade payment for certain joint replacement procedures outside of inpatient settings. After it loosened those regulatory restrictions, such procedures increased in HOPDs and ASCs.2 These advances offer opportunities to expand choice and competition and, ultimately, reduce health care costs without sacrificing quality.
Medicare payment policies and regulatory restrictions continue to preserve site-of-service differentials that unnecessarily encourage lower acuity-services in hospitals. This inflates costs for government and patients alike (since higher prices increase Part B premiums and cost-sharing)3 while exposing patients to adverse events in hospitals, such as the all-to-common hospital-acquired infections.4 It also impacts the overall health care system. Private payers may adopt similar payment policies as Medicare FFS. Additionally, hospital systems sometimes acquire freestanding physicians’ offices and designate them as off-campus HOPDs5 to get a higher payment rate for the same services. This leads markets to become more consolidated, potentially raising prices further.
Recent Policy Actions
In recent years, policymakers have taken steps toward site neutrality. In 2014, Congress passed the Improving Medicare Post-Acute Care Transformation (IMPACT) Act, which set the groundwork for a unified PAC payment system by requiring standardized data reporting from SNFs, HHAs, IRFs, and LTCHs. Additionally, the Bipartisan Budget Act of 2015 (BBA) set site-neutral payment rates, based on the lower rates in the Physician Fee Schedule (PFS) rather than the Outpatient Prospective Payment System (OPPS), for services in “off-campus” HOPDs that were operating prior to enactment of that law.
CMS has also taken regulatory actions to promote Medicare site neutrality. In 2018, it finalized a rule applying PFS-equivalent payment rates to clinic visits at off-campus HOPDs excepted from the BBA. In 2020, the agency finalized policies to permit Medicare coverage of more surgical procedures in ASCs and gradually eliminate restrictions on services that could be performed only in inpatient settings.6 However, the Biden administration reversed those ASC and inpatient-only policies in 2021.7
Further Policy Options
Site Neutrality Between Inpatient and Ambulatory Settings
1: Downsize or eliminate the Medicare IPO list
CMS instituted the inpatient-only (IPO) list to exclude certain procedures from Medicare payment when performed outside of inpatient settings. The IPO list overrides the clinical expertise of doctors and desires of patients. As mentioned above, in 2020, CMS finalized a policy to remove all procedures from the IPO list over a three-year period. Unfortunately, the Biden administration reversed that policy change. Since the IPO list is not in statute, Congress or CMS may eliminate it and allow doctors to decide the site of service based on patients’ individual circumstances, subject to Medicare’s existing safety rules.
Site Neutrality Across Ambulatory Settings
2: Expand the ASC CPL
Medicare will not pay for surgical procedures in ASCs unless they meet the regulatory standards for inclusion on the ASC covered procedures list (CPL). Similar to the IPO list, the ASC CPL’s intent of protecting patient safety prevents doctors from exercising their own judgment to deliver services in lower-acuity and less expensive settings. In 2020, based on stakeholder feedback, CMS relaxed its criteria so that it could add more procedures. In another unfortunate policy move, the Biden administration reversed these changes and instead finalized a process for nominating new procedures through public comment. Expanding CMS’s coverage criteria through statute or regulation would help accelerate the migration of surgical procedures to ambulatory settings when beneficial.
3: Eliminate site neutrality exceptions for off-campus HOPDs
As stated above, the BBA lowered payment for off-campus HOPDs to the PFS rate but exempted most facilities, effectively grandfathering HOPDs billing or under construction as of its enactment in the old payment structure. Eliminating this exemption would align HOPD payment rates and prevent hospitals from exploiting site-of-service differentials by acquiring physician practices and re-designating them as off-campus HOPDs to receive higher payments. Both the Obama and Trump administrations endorsed this policy in their budgets.8
4: Apply physician-equivalent payment rates to certain services in on-campus HOPDs
Services commonly performed in physician offices—such as clinic visits, imaging, or drug administration—have gradually migrated to HOPDs and become their highest-revenue services, as Figure 2 shows.9 Congress’s Medicare Payment Advisory Commission (MedPAC) has recommended reducing OPPS rates or using PFS-equivalent rates for certain services, such as those performed frequently in physicians’ offices or infrequently in emergency departments and those with low patient severity.10 These changes would remove another artificial incentive for hospital consolidation and would reduce outpatient costs in Medicare.
5: Design a unified OPPS/ASC payment system
Another option is to consolidate ambulatory payment systems. OPPS rates exceed those of ASCs, but surgical procedures on the ASC CPL typically have lower complexity and patient severity, which may justify a lower price. Both systems use APCs to categorize services, so it would be relatively straightforward to unify the two. The Trump administration recommended creating a value-based payment program for both facility types.11 Such reforms would be steps toward unifying payment policy for ambulatory care services.
6: Calibrate site-neutral payments for certain services across ambulatory care settings
Setting payment at the lower of the OPPS, PFS, or ASC rate could greatly reduce overpayments, while recognizing that in some cases a HOPD may be the best place to deliver outpatient care despite its higher costs. Policymakers could consider the prevalence or clinical similarity of services in different settings, as discussed by MedPAC,12 and apply the lowest rate to all settings.
Site Neutrality Across Post-Acute Care Settings
7: Implement a unified PAC PPS
Receiving reimbursement under Medicare’s PAC payment systems entails meeting special requirements for each provider type. However, payment differentials for services that can be performed across settings (e.g., rehabilitative care in both IRFs and SNFs) have contributed to overpayments for similar care. Federal agencies and MedPAC have designed a prototype PAC PPS based on clinical needs, case-mix (i.e., patient characteristics), comorbidities, facility type, and geography. They also considered slowing PAC payment updates and creating a value incentive program.13 President Trump’s 2021 budget similarly recommended an episode-based, risk-adjusted PAC PPS based on DRG methodology with a quality reporting program.14
8: Incremental payment reforms for PAC services
Other, smaller PAC payment reforms can also make an impact. For example, the Obama administration recommended reducing payment updates and bundling reimbursement for PAC services. Similar to the proposed PAC PPS, bundled payments could be based on patient characteristics.15 The Obama and Trump administrations also proposed narrowing the criteria for receiving specialized IRF or LTCH PPS rates, thus increasing the use of lower IPPS rates.16
Conclusion
Pursuing site-neutral reforms can yield savings for patients and taxpayers. The Committee for a Responsible Federal Budget has estimated that over ten years, payment reforms across ambulatory settings could reduce federal spending by up to $279 billion, patient costs by $137 billion in Medicare and up to $466 billion in the private sector, and national health expenditures by up to $672 billion.17 Health policy analyst Philip Ellis calculated $231 billion in federal savings, $152 billion in savings for Medicare enrollees, and $117 billion in private premium reductions.18 Individual policies could save taxpayers tens of billions of dollars each, including about $80 billion from post-acute care payment reforms, according to the Congressional Budget Office.19
To be sure, providing more equitable payments across settings of care does not address the underlying tendency for government to misprice health care services. Simply lowering payments across the board is not always optimal and in some cases, it may make sense to offset reduced hospital payments for more intensive or high-cost outlier services. Policymakers should also consider other ways that payment disparities occur between sites of care, such as Medicare paying 340B hospitals for drugs without accounting for the significant acquisition discounts that they receive under law. Overall, site-neutral payment policies are a powerful tool to address concrete instances of overpayments and gaming that policymakers have already identified and reduce incentives for consolidation.20

