
Congressional Democrats are mounting renewed efforts to impose drug price controls. One effort is contained in a new reconciliation proposal. Another, separate measure specifically addresses insulin prices in the INSULIN Act introduced by Senators Jeanne Shaheen (D-NH) and Susan Collins (R-ME). This policy brief examines the INSULIN Act and argues that the proposal will harm patients through higher insulin prices and reduced innovation while raising health insurance premiums and government spending.
Key Takeaways
- The INSULIN Act would increase net prices for insulin. The bill would also increase Medicare and commercial premiums.
- The INSULIN Act misdiagnoses the underlying problem. This misdiagnosis would endanger most diabetic patients and would increase costs for many who are facing already high insulin costs.
- The INSULIN Act would stymie innovation. With at least nine biosimilar insulins available or in the pipeline, imposing price controls now would chill the environment for future innovation in the space.
- The INSULIN Act would burden the federal budget. Due to the increased price for insulin, the bill would substantially increase spending for Medicare and Medicaid.
Insulin Prices in Context
That insulin prices remain top-of-mind for many Americans is unsurprising given current U.S. health trajectories. Over 11 percent of the U.S. population had diabetes in 2019, including nearly 15 percent of adults, and these numbers have been steadily increasing since the turn of the millennium.1
Nearly a quarter of Americans with diabetes require the use of insulin, either alone or with oral medications. These numbers are expected to grow.
Public perception is that insulin prices have been rising, and certain individuals do face relatively high prices. But the majority do not.
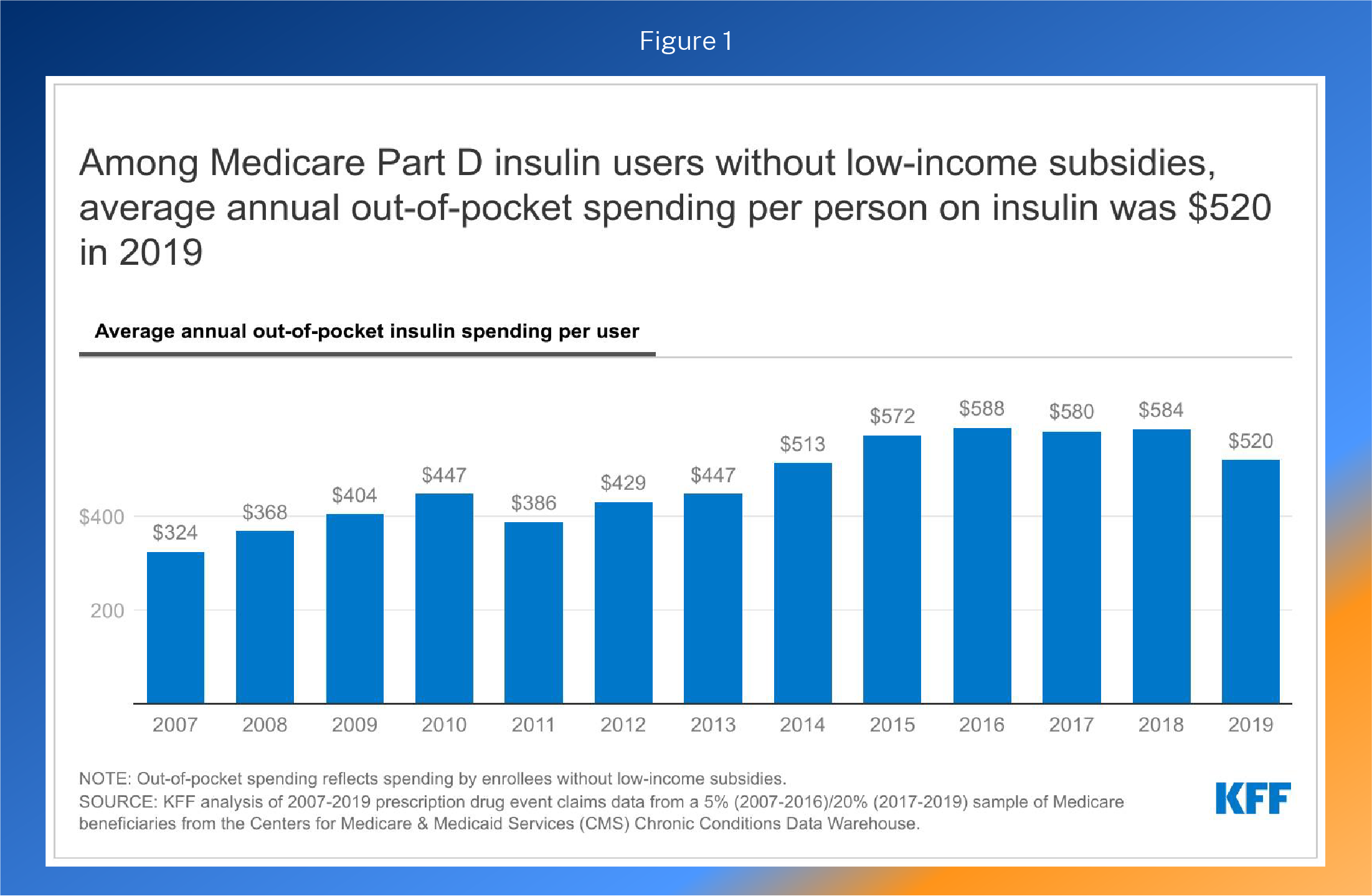
Pharmaceutical price changes are often more visible because people pay more out-of-pocket for drugs. In Medicare alone, Part D enrollees spent nearly $1 billion out-of-pocket on insulin in 2019, four times the amount spent in 2007.2 However, out-of-pocket (OOP) insulin costs in Part D began to fall in 2015. For the trend since 2007, see Figure 1.
This recent trend extends beyond Medicare. Since 2018, OOP costs have fallen across all payers,3 as net prices (what is actually paid after rebates to insurers and pharmaceutical benefit managers) have been declining since 2015.4 In fact, average monthly OOP costs across all payers ranged from $21-$23 in 2021. The average monthly OOP cost has fallen by roughly $8 since 2018. Even list prices (which are sticker prices before discounts) for insulins have begun to decrease5 in a trend that the new and anticipated entries in the biosimilar market will inevitably accelerate.
When considering drug pricing proposals, it is important to understand the difference between list prices and net prices. List prices can be prohibitively high, but most patients never have to face them. In fact, less than 10 percent of individuals with private insurance pay the list price of insulin.6 Even fewer patients enrolled in Medicaid do. Net prices reflect discounts, which are often sizeable, from negotiations between drug manufacturers and insurance plans and their pharmacy benefit managers (PBMs).
That most people face the net price, not the list price, is important to keep in mind when considering the INSULIN Act’s broad policies. When addressing the needs of patients left vulnerable to list prices, particularly within Medicare, policymakers must not enact policies that will increase actual, or net, prices for diabetic patients.
How the INSULIN Act Increases Prices
The INSULIN Act is focused on the list prices of insulin with the idea that lowering list prices, which the Act’s authors aim to do, will reduce out-of-pocket spending. And list prices are less relevant than net prices for most people, including most diabetics.
The INSULIN Act contains three major components. First, the proposal establishes a “voluntary” pricing scheme for drug manufacturers. Second, drug manufacturers can seek to have their insulin products “certified” by dropping their list prices to their 2021 net prices under Medicare Part D. Third, that price would be locked, except for a metric to tie future price growth to general inflation.
While this program is “voluntary,” the bill uses a three-pronged approach to incentivize its uptake. First, insurers would be prevented from receiving price concessions (rebates and discounts) that are typically passed on to consumers through lower premiums for health insurance for “certified” insulin products. Second, cost-sharing for such products would be capped at the lesser of $35 or 25 percent of the (new) list price. Third, certain utilization management tools, such as prior authorization, would be prohibited.
“Certified” insulin products would also have guaranteed placement on formularies under Medicare Part D, Medicare Advantage drug plans, and all private health insurance plans. These mandates, while intended to correct existing market distortions, would instead create new ones—including undermining insurer leverage in price negotiations, preventing plans from promoting cost-effective options, and undercutting competition. These distortions would result in higher premiums for Americans across the board, including among the insulin users whom the bill aims to help.
In short, this bill would lock in prices for insulins based on 2021 market dynamics, grant current insulin market leaders guaranteed formulary placement, and then finance these potentially higher prices by charging all patients higher premiums. All these price distortions would occur at a time when expanded competition from at least nine biosimilar insulins should significantly improve patient well-being and decrease prices (as explained below).
Ultimately, this is a price control bill. However, it’s a particularly perversely constructed price control bill that actually guarantees higher prices by linking to CPI-U for permissible price increases. (A side note: CPIU, as further explained below, has been higher than inflation for prescription drugs over the past decade.) Through price ceilings, the bill risks triggering shortages in both the short- and long-term because the proposed framework effectively de-links insulin pricing from the market realities that impact insulin. Instead of price changes being a function of demand and supply, this framework ties them to general inflation. This type of government control could prove particularly problematic in the event of supply chain disruptions or other drivers of unforeseen surges in production costs, where price increases signal that more supply should go to insulin production.
While the price ceiling would be “voluntary,” it would create strong financial incentives that would have dangerous effects below the surface. In the short term, manufacturers who stand to financially benefit from this new system would likely choose to participate and drive up costs for payers by reducing health plan leverage and obtaining preferred formulary placement. The bill would offer drug manufacturers a guaranteed price that would extend indefinitely into the future and guarantee those products formulary access, thereby reducing the ability of competitors to tend to enter the market. Some manufacturers might use the threat of certification to negotiate higher net prices with PBMs and issuers.
Market Memo: Price Controls
When government sets a maximum allowable price (price ceiling) below the market-clearing price (the price at which quantity supplied equals the quantity demanded), shortages occur. The economics are similar to those caused by a tax on the industry–whereby the government arbitrarily makes certain products less profitable than they would otherwise be. The business responds to the regulations by cutting production, reducing quality, and shifting costs elsewhere. These actions clearly harm consumers.
The shortages caused by the government’s price controls lead businesses to reduce or even stop production, as investments in the price-controlled product are artificially disincentivized. In the case of a price ceiling, production that could have occurred is simply lost – never to occur due to government regulation. Actions taken in response to that artificial information perpetuate a distorted market.
The Congressional Budget Office (CBO) estimates that the bill would “increase in the average net price of insulin resulting from the certification process.”7 The resulting increased costs would cost Medicare $8.2 billion over a ten-year period and increase the federal deficit by $23.3 billion over the same period.
The “voluntary” nature of the framework also creates an uncertain environment for future innovation. Congress could use the INSULIN Act’s bureaucratic model as the basis for more sweeping pharmaceutical price controls in the future – such as making the insulin program compulsory in the future or expanding it to other categories of drugs.
The cap on out-of-pocket expenses would simply force insurance companies to increase premiums. It is important to consider that health insurers try to spread costs among members. When a federal mandate requires that a plan charge less for a certain product, other plan members foot the bill through higher premiums.
How the INSULIN Act Undermines Innovation
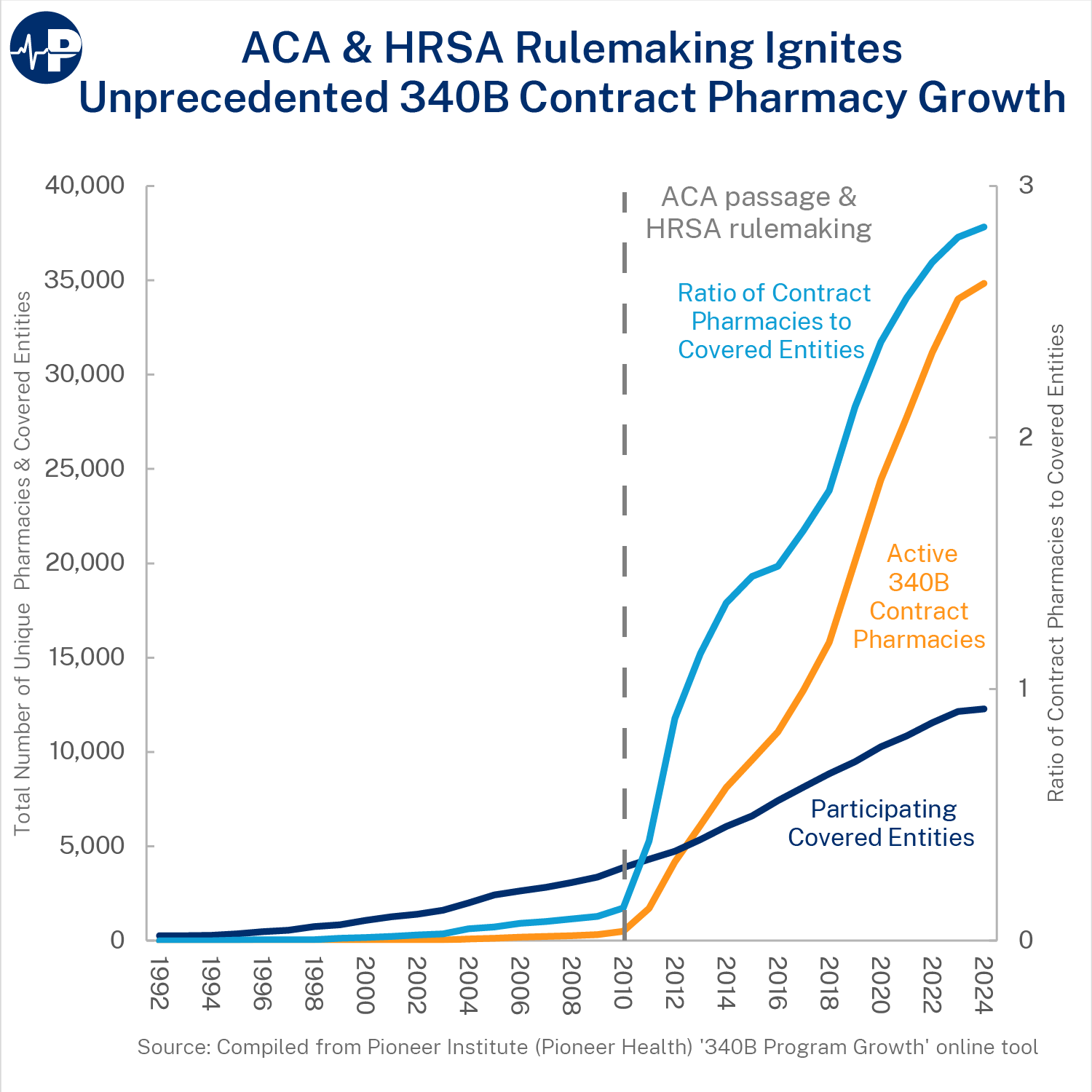
Insulin innovation has been substantial over the last 100 years. The insulin used today has changed substantially since its discovery in 1921. The discovery of insulin analogs has led to better management through tools such as insulin pumps, pens, and inhalers. The next frontier for insulin innovation is the introduction of biosimilar insulins. Biosimilars function similarly to generics for biologic products such as insulin. A biosimilar pathway was created by the Affordable Care Act, but it is only recently that biosimilar insulins have reached the market. Now that biosimilar insulins can meet FDA approval, there are already two FDA-approved biosimilar insulins with at least seven8 more in the pipeline.
Biosimilars have the potential to improve competition in the insulin market and drive down prices. The INSULIN Act would stymie this type of innovation. By locking in the current pricing structure for insulin, there would be two negative incentives: 1) current market leaders would lock in favorable formulary placement at current prices, reducing the incentive for price competition from biosimilar competitors; 2) the price ceiling would lessen incentives to create better insulin products. In doing so, not only would prices for biosimilars remain stagnant, but brand name prices would also remain stagnant due to less downward pressure from biosimilars in future years. Biosimilars can cost between $100 to $300 million to develop.9 Reducing their ability to compete with existing products would likely lead to many fewer products coming to market.
While the quality of insulin would be negatively affected, the price patients pay for insulin in the future would necessarily increase because of this effect. The INSULIN Act would guarantee that in the long term, prices would become and remain artificially high because of the reduction in biosimilar competition and the distortive price ceiling. This reality is particularly troublesome at the very beginning of biosimilar innovation expansion.
The effect on innovation goes beyond the insulin market, however. As discussed, price ceilings can produce shortages. Those shortages could occur throughout the pharmaceutical industry as necessarily less capital flows into it.
Other considerations
One overlooked consideration stems from a policy in the American Rescue Plan Act that lifts the cap on Average Manufacturer Price (AMP) rebates within Medicaid beginning in 2024. Removing the cap will lead to larger rebates for certain drugs with rising list prices, including a sizable number of insulin products.10 By artificially lowering the list prices for drugs, the INSULIN Act will likely result in lower rebates for many states’ Medicaid plans. CBO confirmed this in its analysis, estimating that the bill would increase Medicaid spending by $7.7 billion over a ten-year period due to lower rebates. This situation would create two economic distortions within the already flawed Medicaid Drug Rebate Program, which sometimes forces drug manufacturers to pay Medicaid to place their drugs on formularies. Policymakers should work to fully understand the impact that provisions in the INSULIN Act would have on such plans and what effect inserting yet another artificial distortion into federal health programs would have on patients.
Further, the pricing scheme used in the bill deserves closer scrutiny. Tying the price of insulin to any inflator is problematic as it would create an arbitrary metric divorced from consumer preferences and market conditions. CPI-U, the inflator which the scheme adopts, is an especially poor fit during explosive CPI-U growth that has dwarfed increases in prescription drug prices, particularly over the past year. In fact, tying price increases to CPI-U would drastically inflate consumer costs for many products, further straining family finances.
Conclusion
As policymakers consider the INSULIN Act and other drug pricing proposals, they must fully understand the effects such proposals would have on patients who rely on the drugs. In this case, innovators are on the verge of bringing several biosimilars into the market.
Proposals must enhance such competition, not stymie it as this bill would do. Government-erected barriers to competition and innovation would reduce access to care and increase costs. Moreover, this proposal harms patients with higher prices and premiums and harms taxpayers with higher costs of federal programs.
The INSULIN Act cannot be viewed in a vacuum. That is as true for its policies, which affect the entire economy, as it is for its timing, given the current push to enact sweeping drug pricing legislation through reconciliation. The price controls used in the INSULIN Act are a precursor to the wider controls featured in the reconciliation bill. Both proposals would fail to do what naturally brings down prices: enhancing competition. Both proposals would also inhibit the flow of capital needed to bolster the ecosystem that produces the remarkable innovation American patients have enjoyed for decades.