




As Americans face rising inflation1 and recession risk,2 Congressional Democrats have proposed a misguided budget reconciliation bill focusing on health care. The legislation would set price controls on prescription drugs and limit price increases to the rate of inflation. It would extend elevated Affordable Care Act (ACA) subsidies—enacted under the American Rescue Plan and set to expire after 2022—for at least two more years. The legislation purports to reduce the deficit, but much of the “paper” savings result from the budget gimmick of repealing a Trump-era drug rebate rule that has been challenged in court, delayed by the Biden administration, and will likely never go into effect.
The reconciliation bill would harm patients and taxpayers. The drug price controls would decrease the number of innovative drugs developed, thereby diminishing Americans’ quality and length of life. The insurance subsidies would expand federal spending without enacting any meaningful reform to a broken system. Critically, both proposals would incite inflationary pressure when inflation is already at a 40-year high.
Key Takeaways
- The reconciliation bill would harm patients and lower American life expectancy and the quality of life by reducing pharmaceutical investment and the number of innovative, life-saving drugs.
- The reconciliation bill would induce drug shortages and higher launch prices for some medications.
- The reconciliation bill would benefit the wealthy and health insurers with much higher ACA subsidies.
- The reconciliation bill would increase inflationary pressures by replacing private spending with government spending.
- The reconciliation bill includes major budget gimmicks, making it unlikely to reduce federal deficits.
Drug Price Controls
The reconciliation proposal would address drug prices in three ways.3 First, it would allow the Secretary of Health and Human Services (HHS) to “negotiate” prices for a limited number of prescription drugs. Second, it would require drug companies to pay rebates if they increase their Medicare and commercial prices faster than inflation. Finally, the bill would limit Medicare beneficiaries’ annual out-of-pocket Medicare Part D drug costs to $2,000.
This bill is the third recent Democratic drug pricing proposal. Each allows the HHS Secretary to directly “negotiate” with drug makers by revoking the provision in the Part D statute that prohibits the HHS Secretary from interfering in negotiations between private Part D plan sponsors and drug makers. Currently, in Part D, insurers compete on benefits and prices and negotiate discounts to keep costs down, and costs have consistently been below projections.
In reality, there would be no meaningful negotiation under the Democratic proposal. The secretary would have all the negotiating leverage. The proposal states that the Secretary’s determination of negotiation-eligible drugs would not be subject to administrative or judicial review. And companies that fail to negotiate to the Secretary’s satisfaction or adhere to the Secretary’s set price would be subjected to confiscatory penalties—an excise tax up to 95 percent of sales of the drug. The Secretary would be making price “offers” that manufacturers could not refuse.
Bad Policy for an Overstated Problem
The legislation builds on the commonly held misconception that prescription drug prices are rapidly increasing. The legislation’s proponents have focused on increases in drugs’ list prices. While small numbers of patients bear a disproportionate burden from list prices, the “net” prices most Americans pay after rebates and discounts are considerably lower.
General inflation is alarming: prices are up 9.1 percent over the past year.4 Yet even in this period of supply chain disruptions and widespread shortages, drug inflation is up just 2.5 percent year-to-year.
In fact, total drug spending growth has been stable the last 15 years and has been much lower than the growth in health care spending.5 Low drug price inflation is the result of rebates, discounts, and increased drug approvals, especially generics that increase competition. While prices of a relatively few branded, specialty medicines are extremely high, Americans use more generics (9 out of 10 prescriptions) and pay less for them (16 percent lower on average) than patients in other developed nations.6
Shortages and Higher Launch Prices
The proposal would also require manufacturers to rebate price increases on their Medicare and private market drugs that exceed general inflation. Setting artificial caps on price increases would distort market mechanisms that reflect the value added of a drug. Price increases for drugs with high or growing value are a signal to producers to increase supply. Limiting that increase could result in shortages that impair some patients’ health.
The Congressional Budget Office (CBO) analyses of these types of inflation controls have said they might induce higher launch prices for new drugs.7 Currently, manufacturers might temper their launch prices for a variety of reasons, including to gain market share or to aid a vulnerable patient population, if they are confident of being able to subsequently raise prices to match market conditions. But with the proposed limits on price increases, manufacturers would be less likely to moderate launch prices. This would likely increase list prices and possibly even net prices for some new drugs. This could result in higher out-of-pocket payments—normally based on list prices—for insured patients and higher actual prices for patients without drug coverage who are stuck with list prices. Some of these people will end up forgoing treatments because of increased costs.
This would affect the very drugs that are the most innovative and valuable for improving health. For example, new gene therapies may yield a cure for sickle-cell disease. The disease disproportionately affects low-income and minority populations. Higher launch prices might put these life-saving treatments out of reach for these vulnerable populations.
A Faulty Methodology that Could Harm Patients with High Use Drugs
The proposal would direct the HHS Secretary to negotiate the price of sole source drugs on which Medicare spent the most during the preceding year. But high expenditures can result from high prices or high usage. In other words, a high-use drug would likely be subject to negotiation, regardless of whether its price was unreasonably high. This could depress drug supply and harm patients.
In fact, recent growth in total retail pharmaceutical spending was driven by volume, not prices, which decreased by 1.0 percent in 2018 and 0.4 percent in 2019. Even in 2020, the first year of the pandemic, total retail prescription drug prices continued to fall by 0.1 percent.8
Harm to Patients by Decreasing the Number of Life-Saving New Drugs
Innovative, new drugs effectively decrease the price of health by reducing the need for other medical services and by extending and improving the quality of life. For example, new HIV drugs transformed a uniformly fatal disease that could not be effectively treated at any price into a chronic condition. New Hepatitis C drugs cured a life-threatening and debilitating disease that was previously poorly treated using expensive drugs with severe side effects.
Drug development is a risky and expensive business. The process normally takes ten years or more. Only about one-in-ten products make it to market. Once failures and the cost of capital are calculated, the costs per success are in the billions. Pharmaceutical companies invest in research and development in anticipation of future profits. They will decrease investment if future profits are limited by government.
A systematic review of published academic studies between 1995 and 2020 showed a significant negative relationship between drug price controls and both investment in pharmaceutical research and development (R&D) and access to innovative drugs.9 For every 10 percent decrease in prices, there was a 5 to 6 percent decrease in R&D investment leading to decreased future drug discovery. And countries with drug price controls suffer drug launch delays and decreased access to new drugs compared to the U.S.10
The Council of Economic Advisers estimated that the first version of the Democrats’ proposal—H.R. 3, the Lower Drug Costs Now Act of 2019—would lead to as many as 100 fewer new drugs available to Americans over the next decade.11 That is about a third of the total number of drugs currently expected to enter the market. This decreased access to drugs would reduce Americans’ average life expectancy by an estimated four months.
University of Chicago economist Tomas Philipson estimated that the second version of the Democrats’ proposal—the Build Back Better bill—could lead to a 29 to 60 percent reduction in R&D and 167 to 342 fewer new drug approvals over the next 20 years.12
The price controls in the current reconciliation proposal would be just as destructive. By limiting new R&D investment, the bill would decrease the number of innovative new drugs that improve health, extend life, and eventually become the low-priced generics used by most Americans.
Limiting price increases to the level of inflation would also damage innovation and harm patients. Economists estimated that if controls had limited the growth rate of U.S. drug prices to the rate of inflation, R&D spending would have been 30 percent lower, resulting in 330-365 fewer new drugs—38 percent of all new drugs marketed worldwide—coming to market between 1980 and 2001.13
More Subsidies for Insurers
The second main component of the proposed reconciliation package would continue the misguided policy of obscuring the unaffordability of ACA plans with increased taxpayer subsidies to health insurers. The ACA’s insurance mandates caused premiums and deductibles for individual market coverage to soar. In 2020, the average family plan carried a combined premium and deductible of $25,000,14 and the average plan provides access to far fewer providers than group plans.15 Most enrollees receive large subsidies—referred to as premium tax credits (PTCs)—that substantially reduce their share of the premium. The ACA’s PTCs limit the percentage of income that households pay for a benchmark plan (the second-lowest cost plan available in the exchange). The PTCs phase out as household income increases and were capped at 400 percent of the federal poverty level (FPL).
Rather than reform the underlying program, which has resulted in such unattractive plans, congressional Democrats have focused on increasing subsidies. In the American Rescue Plan (ARP) Act, Congress made the subsidies for 2021 and 2022 more generous by reducing the maximum percentage of income that households must pay for a benchmark plan and by expanding eligibility to people with incomes above 400 percent of the FPL. This caused a surge of Obamacare spending. CBO estimates that the expanded subsidies will cost about $30 billion in 2022.16 The expanded subsidies are poor public policy.
Unfair Benefit for Wealthy Households
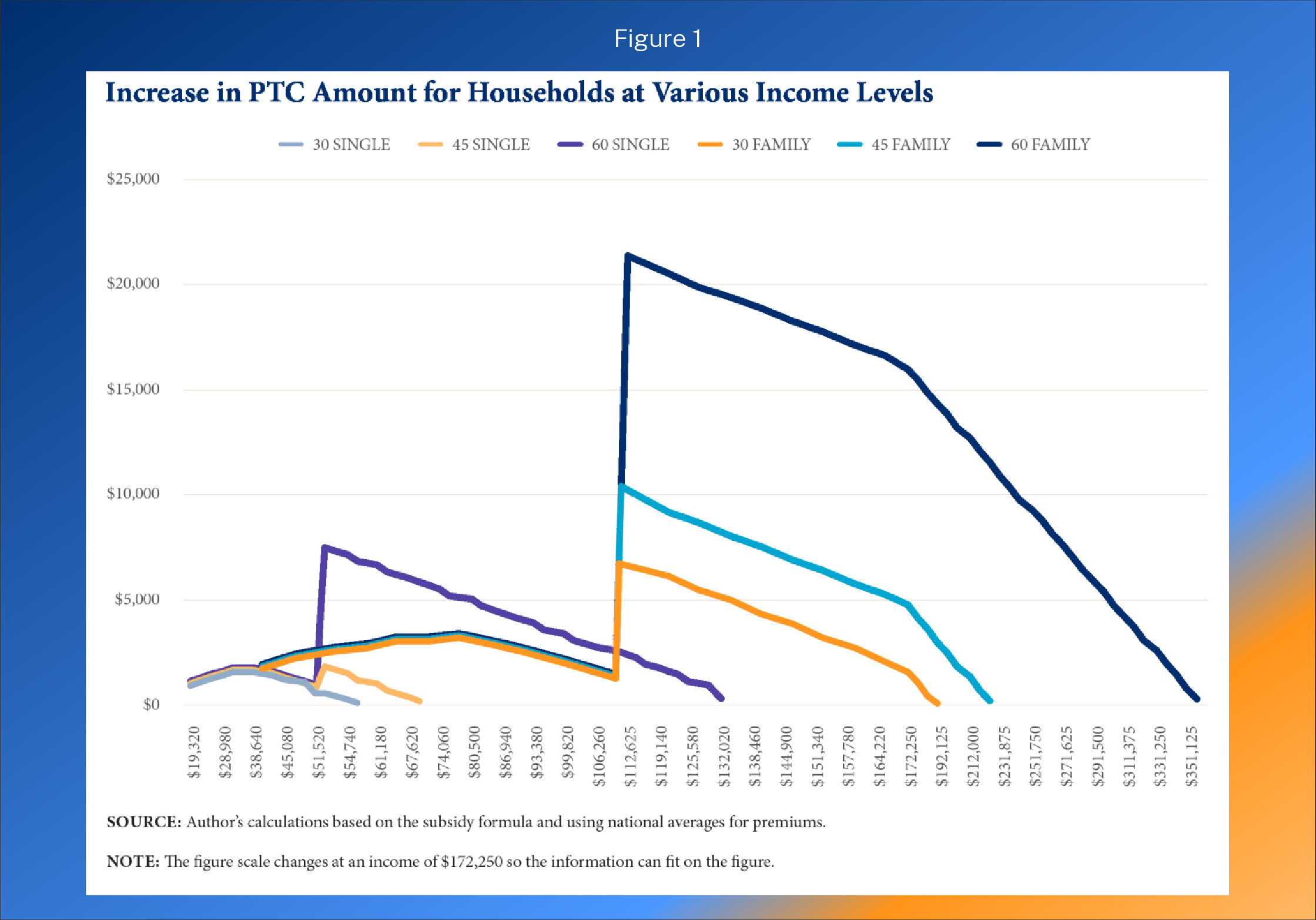
The largest benefit of the expanded subsidies accrues to households with income above 400 percent of the FPL. The benefit is also larger for older households and households in higher premium areas since the subsidy structure limits premiums to a certain amount based on household income, regardless of the age of the household members or the actual premium.
On average, in 2021, a family-of-four headed by a 60-year-old qualified for a $21,327 subsidy if they earned 401 percent of the FPL. If that household earned eight times the FPL—or $212,000—the subsidy exceeded $12,000. In some parts of the country, households with incomes of more than $500,000 qualified for subsidies in 2021 and 2022. For example, in 2021, a 64-year-old couple with no dependents in Kay County, Oklahoma and an income of $500,000 per year, faced a benchmark premium of $49,897 and qualified for a subsidy of $7,397.
Crowd Out of Private Financing and Increased Inflation
CBO originally estimated that nearly 75 percent of the spending on the expanded subsidies was for individuals who already had health insurance—either existing exchange enrollees or new exchange enrollees who previously had another source of coverage.17 In other words, most of the new government spending simply replaced household spending, permitting these households to spend more in other ways. This contributes to inflation by increasing aggregate demand without an increase in aggregate supply.
Higher Health Care Prices and Higher Premiums
The ACA’s subsidy design gives insurers pricing power since almost the entire premium increase is paid by the government. The ARP’s expanded subsidies worsened the problem by making the subsidies even more expensive and bringing more households into the perverse structure. According to CBO’s May 25, 2022, report, premiums for exchange plans are rising faster than they anticipated, as are the subsidies.18
In Focus: West Virginia
If the enhanced PTCs expire after 2022, the largest per person subsidy loss is for people with income above 400 percent of the FPL. Not many exchange enrollees in West Virginia have income above 400 percent of the FPL. According to estimates from University of Minnesota economist Steve Parente, fewer than 1,200 West Virginians with income above 400 percent of the FPL are currently enrolled in the exchanges
Loss of Employer Coverage
The ACA subsidies are not available to households with an offer of affordable employer coverage. As the size of the subsidies increase, so does the incentive for employers to not offer coverage. Small employers—those with fewer than 50 full-time employees—will be particularly incentivized to not offer coverage since they are exempt from the employer mandate tax penalties.
Benefiting Insurers, Not Consumers
The ACA subsidies are sent directly from the U.S. Treasury to health insurance companies. A recent economics study found consumers value the subsidies at less than half of their cost.19 This study found that the big winners from the flawed subsidy design are health insurers, confirming earlier studies that show that health insurer profits soared after the ACA took effect.20
Perpetual, Costly Problem
The ARP’s two-year expansion of the ACA subsidies was designed as a temporary, pandemic relief measure. In Washington, short-term extensions of government spending programs, which generally foreshadow additional temporary or permanent extensions, are a budget gimmick to keep the perceived cost of the legislation down. A permanent extension of the expanded subsidies would be very expensive, partly because of much greater decline of employer-provided coverage which has a much lower budgetary cost than the ACA PTCs. According to CBO’s estimates, a ten-year elevated subsidy extension would increase deficits by $248 billion—$306 billion in PTC costs offset by $67 billion in higher federal tax revenue.21
Conclusion
The reconciliation proposal being considered in Congress would do far more harm than good. The proposal would increase government power over Americans’ health care. It would add inflationary pressures by raising health insurance premiums and costs during an inflation crisis. Worse, the proposal would subsidize the insurance industry and wealthier Americans at the cost of life-saving cures. The bill’s drug pricing control mechanisms are unnecessary and would diminish Americans’ health by decreasing the number of innovative, life-enhancing drugs in the future. If they precipitate an increase in new drugs’ launch prices, they will exacerbate rather than alleviate high drug prices.
Much of the projected budgetary savings from the bill are illusory, paper savings that result from the repeal of a Trump-era rebate rule that is unlikely to ever go into effect. And the two-year elevated ACA subsidy extension is another gimmick.
Rather than legislation with poor policy and budget gimmicks, policymakers should instead look to policies that empower patients, reform underlying problems in government programs, and ensure Americans are not left more vulnerable to inflation eating away at their incomes and savings.

