
Brian Blase, Ph.D.
Brian Blase, Ph.D., is the President of Paragon Health Institute. Brian was Special Assistant to the President for Economic Policy…
Reforming Government, Empowering Patients
Navigation
This paper outlines strategies to reduce U.S. federal health spending, focusing on reforms in Medicaid and Medicare to prevent future tax increases or benefit cuts, advocating for a sustainable fiscal trajectory through targeted policy changes and efficient program management.
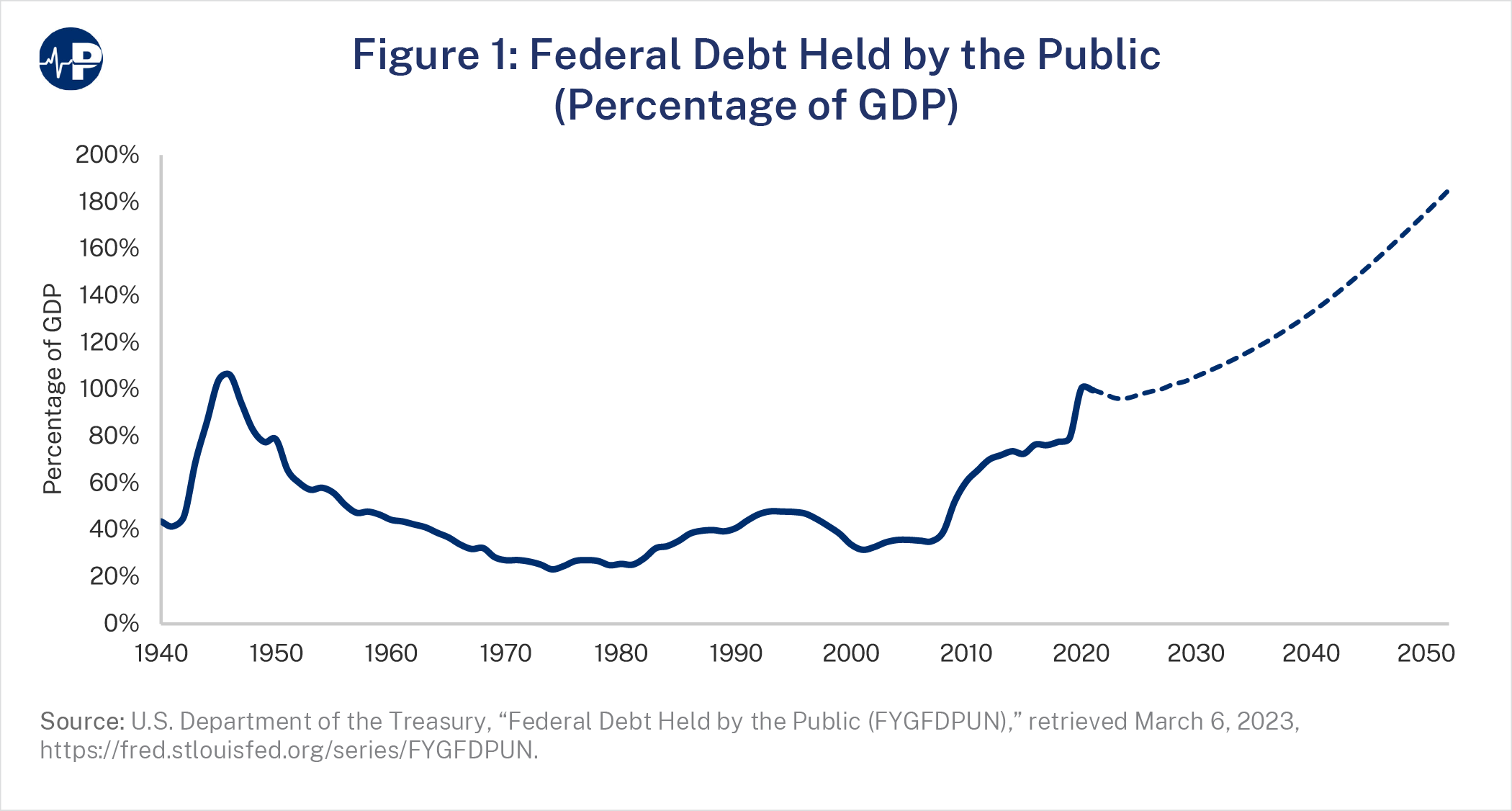
Federal debt now tops $31 trillion.1 As a percentage of the economy, federal debt is the highest since World War II. Annual deficits, projected at $1.4 trillion this year, are expected to reach nearly $3 trillion in the next decade.2 Higher federal spending, deficits, and debt have contributed to the 40-year-high inflation and rising interest rates Americans are now experiencing.3
The problem is worsening as the Congressional Budget Office (CBO) expects cumulative federal deficits to exceed $20 trillion over the next decade,4 up more than $4 trillion from its estimate just nine months prior.5 CBO’s rising deficit projections result from new federal spending and higher interest rates, which makes past debt more expensive. But the biggest driver of the U.S. structural fiscal imbalance is spending on mandatory health programs, including Medicare, Medicaid, and subsidies under the Affordable Care Act (ACA). Within 30 years, these programs will grow from about a quarter of non-interest federal spending to about 40 percent, and from 6 percent to 9 percent of the economy.6
Even a country as wealthy as the United States will eventually face severe consequences if federal debt continues to escalate as a percentage of gross domestic product (GDP). Persistently high federal deficits will increase interest payments for past borrowing and in turn make it harder to sustain the country’s debt load. CBO projects that net interest spending will be $640 billion in fiscal year (FY) 2023.7 According to CBO, net interest payments would exceed $1.4 trillion in FY 2033 assuming that inflation remains low by historical standards and average interest rates on 10-year notes are below 4 percent.8 If CBO’s assumptions prove too optimistic, the burden of debt could be much greater.
In a February 2023 Paragon paper, budget expert Paul Winfree wrote that the government could exhaust its capacity to take on additional debt as soon as 2045 and that the “only way to shift course is to make meaningful reductions in federal health spending … within the next decade.”9 Winfree estimates that policymakers need to reduce federal health spending by roughly $1.6 trillion, relative to baseline, over the next decade to put it on a sustainable trajectory and avoid massive fiscal pain—large tax increases and benefit reductions—in the future. The reforms presented in this paper would collectively save more than that amount. Passage of such reforms would demonstrate that policymakers prioritize the future prosperity of the country.
The unsustainability of federal health programs has been known for some time. During a White House health care summit in February 2010, then-President Obama remarked:
We’ve got some people who’ve been working a very long time on figuring out how can we control the huge expansion of entitlements. Almost all of the long-term deficit and debt that we face relates to the exploding costs of Medicare and Medicaid. Almost all of it. That is the single biggest driver of our federal deficit. And if we don’t get control over that we can’t get control over our federal budget.10
In the 13 years since those remarks, the problem has only worsened, particularly given the aging of the population and the decline in the number of workers supporting program beneficiaries. Simple mathematical realities indicate that delaying reforms will necessitate large benefit cuts or massive tax increases in the future.11 Alternatively, timely action would allow for more gradual reforms that do not disrupt benefits.
In this paper, we present options to reduce federal health spending primarily through reforms to Medicaid and Medicare. While there is much to improve in these programs, the proposals in this paper do not necessitate sweeping restructuring of them. Many of the proposals have a history of bipartisan support and have been proposed by CBO or the Office of Management and Budget (OMB) numerous times.12 Furthermore, many reforms that reduce federal health spending can directly benefit Americans by reducing out-of-pocket costs.13 Every proposal in this paper has been estimated to individually save the federal government at least $10 billion over 10 years. In total, we present 12 proposals that would total $2.1 trillion in potential savings over a decade. The estimated savings would be hundreds of billions of dollars greater if they included reduced interest payments from lower spending and if CBO updated its calculations of older proposals.14
The federal government provides an open-ended reimbursement of state Medicaid expenditures, which means that states receive more federal money when they spend more on Medicaid. The reimbursement rate for traditional Medicaid populations (i.e., low-income seniors, individuals with disabilities, children, and pregnant women) varies by state per capita income. Wealthier states typically receive a 50 percent reimbursement (the federal floor), and the poorest states receive about a 75 percent reimbursement. The federal reimbursement percentage is referred to as the federal medical assistance percentage (FMAP). The ACA expanded Medicaid to able-bodied, working-age adults, with a much higher reimbursement rate (90 percent) for these enrollees in states that adopted the expansion.
This open-ended federal reimbursement has produced explosive Medicaid growth, with federal Medicaid spending up from $35.5 billion in 1989 to $592 billion in 2022.15 The lack of clear accountability between states and Washington has also led to an extremely high improper payment rate, which has exceeded 20 percent of federal program spending, even with incomplete audits.16 The open-ended reimbursement also gives states an incentive to create artificial expenditures—which the federal government permits within certain limits— to obtain federal funds without actually putting up state dollars.17
To meaningfully improve fiscal responsibility in Medicaid, restore the integrity of the federal-state relationship, and better ensure value from the spending, this open-ended reimbursement structure needs to be replaced. Such a change would be major reform and would take time to properly develop. As a start, however, Congress could take several meaningful steps to reduce wasteful Medicaid spending and better align state incentives to improve the value of their programs.
Now is an ideal time to consider such reforms because of the combination of large and growing federal deficits with large state surpluses and reserves.18 The U.S. Census Bureau reports that states had $6.6 trillion in cash and security holdings in 2021, up 20 percent from the previous year.19 Federal COVID policy, which delivered hundreds of billions of dollars to states in direct support and higher Medicaid payments as well as unprecedented income support for Americans and American businesses, has contributed to states’ strong fiscal situation. From this position, states have generally pursued inflationary fiscal policy over the past few years, enacting tax cuts and increasing spending, including continued direct cash payments.20
Eliminate Medicaid Provider Tax Safe Harbor
Medicaid provider taxes are the only tax that the ones paying it, which are most often hospitals or nursing homes, lobby the state government to assess on them. The reason: it’s not a real tax; it’s more a legalized kickback. States and providers have agreements in which the state uses the tax revenue obtained from the provider to pay those same providers through higher Medicaid payments. In the process, the state obtains federal reimbursement for those expenditures. The state then uses a portion of that reimbursement to increase payments to those providers. Thus, the state and the providers receive a windfall at the expense of federal taxpayers.
From 1989 to 1993, there was a surge in provider tax use, and federal Medicaid spending increased by an average of 20 percent annually.21 Congress responded by requiring that provider taxes be charged at uniform rates on all providers of the same type.22 Congress also prohibited states from establishing hold-harmless arrangements to compensate for taxes on providers with increased Medicaid payments to those same providers.23 This action was supposed to limit the outright quid pro quos involved. However, there is a “safe harbor” exception that allows states to use hold-harmless arrangements so long as the tax does not exceed 6 percent of a provider’s net revenues from treating patients. In other words, so long as the tax rate does not exceed 6 percent, states can still funnel payments to politically favored providers through the provider tax financing scheme.
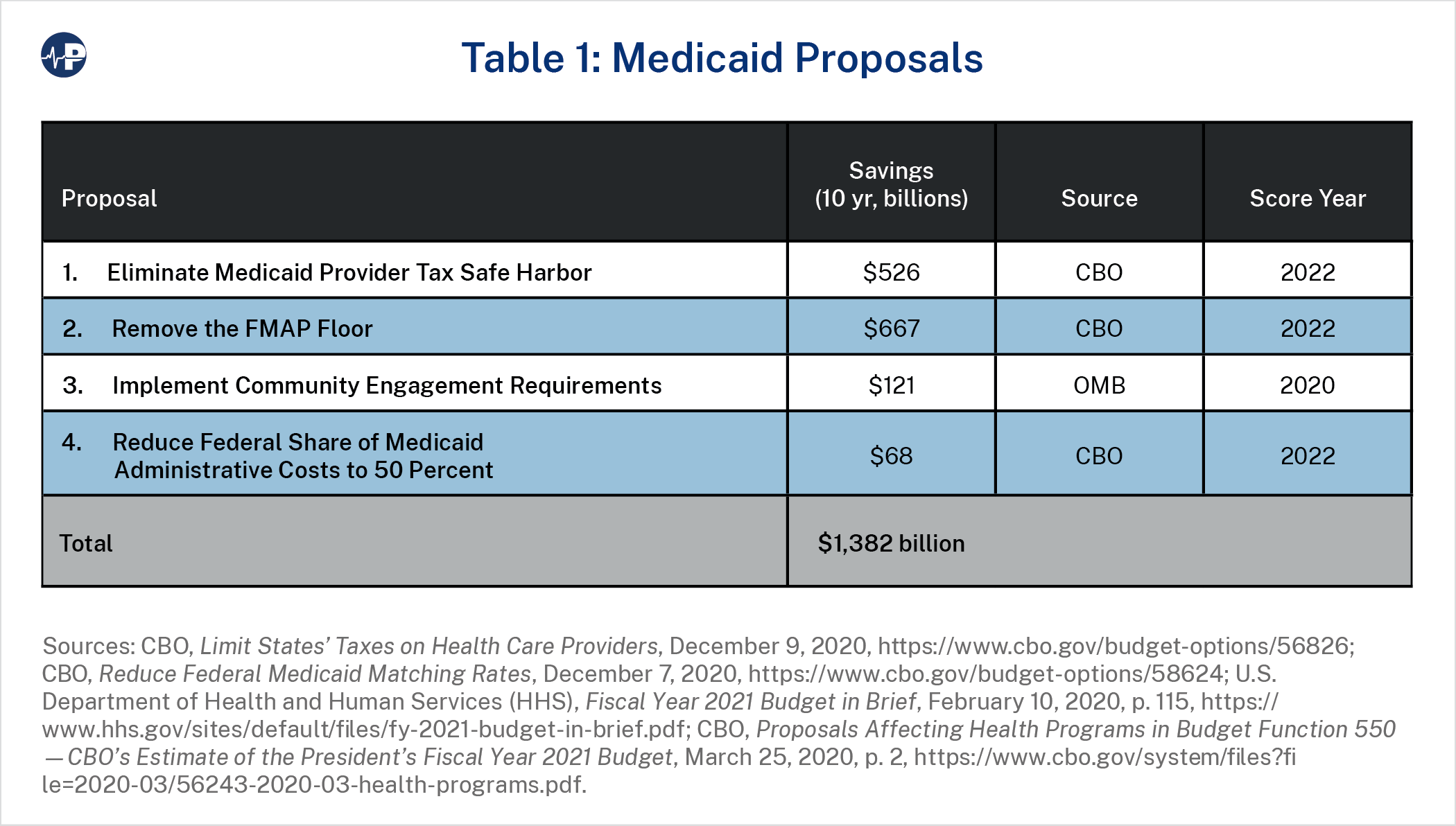
CBO estimates that eliminating the safe harbor threshold would save $526 billion over 10 years. CBO also analyzed reducing the safe harbor threshold to 5 percent and 2.5 percent, projecting respective budgetary savings of $41 billion and $209 billion.24 Importantly, states could still have provider taxes, but states would not be able to establish schemes that protect and enrich certain providers with higher Medicaid spending raised through the tax.
CBO estimates budget savings because it assumes that states would replace only about half of the lost revenues with real state Medicaid contributions. In essence, states would determine that a part of their current Medicaid spending was not providing value relative to other priorities when the full cost could not be passed on to the federal government. Federal savings would be smaller from provider tax reform if states replace more of the revenue from the provider tax scheme and lower if states replace less of the revenue.
In the past, bipartisan leaders at the highest levels of government have supported provider tax reform. During the budget deficit talks in 2011, then-House Majority Leader Eric Cantor raised the issue of provider taxes, and then-Vice President Biden agreed that eliminating them was sound policy. Cantor led the Republican negotiators, and Biden led the Democratic negotiators. Here is an excerpt from Bob Woodward’s The Price of Politics that begins with Cantor raising the issue:
“What about the Medicaid provider tax?”
It’s a scam, Biden agreed. The states were gaming the system, taxing doctors and hospitals so they could get federal reimbursements and then returning the money to the
providers. Let’s call it like it is, and let’s just do this. For a moment, Biden sounded like a Republican. It could save $40 billion. “If we can’t do this—” the vice president said,
“come on!” …
We’re going to do lots of hard things, Biden said. … We might as well do this, he said. The administration would adopt the Republican view on this.25
Remove the FMAP Floor
Although the FMAP structure appears to favor poorer states over wealthier states, the reality is that wealthier states tend to receive far more federal Medicaid funding than poorer states because wealthier states have had the fiscal capacity to grow larger programs. For example, in 2019, New York (state per capita income: $67,366) received $17,145 in federal Medicaid funding per person in poverty, while Alabama (state per capita income: $43,288) received $6,148 in federal Medicaid funding per person in poverty. Congress has further advantaged wealthy states by creating an FMAP floor of 50 percent for traditional enrollees, which guarantees them a relatively high level of funding—proportionately more than they would have received were their FMAPs, like those of poorer states, based strictly on per capita income. Removing this floor has been a part of Medicaid reform discussions for more than a decade.26
According to CBO, removing the floor would affect 13 states and would save $667 billion over a decade. CBO anticipates that these savings would not come from states’ limitations on eligibility but instead through other changes that lower state spending, such as reducing the number of optional medical services.27
Implement Community Engagement Requirements
The expansion of Medicaid over the past decade has shifted the program from its traditional focus on the neediest Americans. The Trump administration’s FY 2021 budget proposed requiring this subset of able-bodied, working-age Medicaid enrollees to engage in employment, training, or community service in order to be enrolled in the program. This would better focus Medicaid on those whom the program was intended to serve as well as improve communities and bring Medicaid into alignment with other federal public assistance programs that have similar requirements. CBO estimates that this budget proposal would save roughly $121 billion.28
Reduce Federal Share of Medicaid Administrative Costs to 50 Percent
The federal government’s share of administrative expenses varies by category of costs. It covers half of general administrative expenses, but for other expenses it can range from 70 percent to 100 percent. Combining all these categories, the overall average federal share of administrative expenses was 62 percent in 2021, according to CBO.29 This amounts to $20 billion, or about 4 percent of total federal Medicaid spending.
CBO estimates $68 billion in federal savings from moving the federal share of administrative spending to 50 percent for all categories.30 Such a change would likely reduce some administrative complexities and limit state gaming to move administrative expenses to areas that receive higher reimbursement. Given the large federal budget deficits and large state surpluses, such a change would be commonsense governing.
Medicare is the single largest federal health program in terms of spending. As such, its payment rules have a significant impact on the health care system as a whole. Critics of entitlement reform often claim that savings would come at the expense of seniors, but there is a great deal of inefficient spending in the program that should be reduced and would not harm access to services. For example, provider payments are a major component of Medicare spending, and higher inpatient and outpatient costs in particular drive higher U.S. spending relative to other countries.31
A key issue is ensuring that Medicare savings actually improve the program’s finances. Twice in the past 13 years Congress has significantly reduced Medicare spending relative to baseline. The ACA reduced Medicare Advantage (MA) payments. The Inflation Reduction Act (IRA) allowed the Secretary of Health and Human Services (HHS) to reduce what Medicare pays for prescription drugs. However, spending reductions in both cases were not used to shore up Medicare’s finances but for other priorities.
One benefit of certain Medicare payment reforms is that federal savings often result in lower premiums and cost-sharing for Part B beneficiaries. Lower spending in traditional Medicare also leads to savings in the MA program due to benchmark calculations.32
Modernized Program Design
In traditional fee-for-service (FFS) Medicare, beneficiaries pay monthly Part B premiums and separate deductibles for Part A and Part B (hospital and medical insurance benefits, respectively), as well as other cost-sharing requirements.
The vast majority of FFS enrollees have supplemental coverage to reduce these expenses, with relatively wealthier enrollees purchasing Medigap plans that charge monthly premiums roughly equal to those of Part B premiums.33 Supplemental coverage essentially eliminates cost-conscious behavior, generally by making care “free” at the point of service, and thus increasing total Medicare spending by 22 percent to 27 percent.34 MA plans reduce beneficiary cost-sharing to attract enrollees as well. However, unlike Medigap plans, MA plans must deliver a full package of Part A, Part B, and sometimes other benefits, meaning that they must bear the total cost of covering benefits in addition to any cost-sharing reductions they choose to provide. Supplemental Medigap plans do not cover core Medicare benefits, so their coverage of cost-sharing changes beneficiary behavior by encouraging them to consume more services due to lower cost-sharing, without the Medigap plans bearing the resulting additional costs that they indirectly encourage.
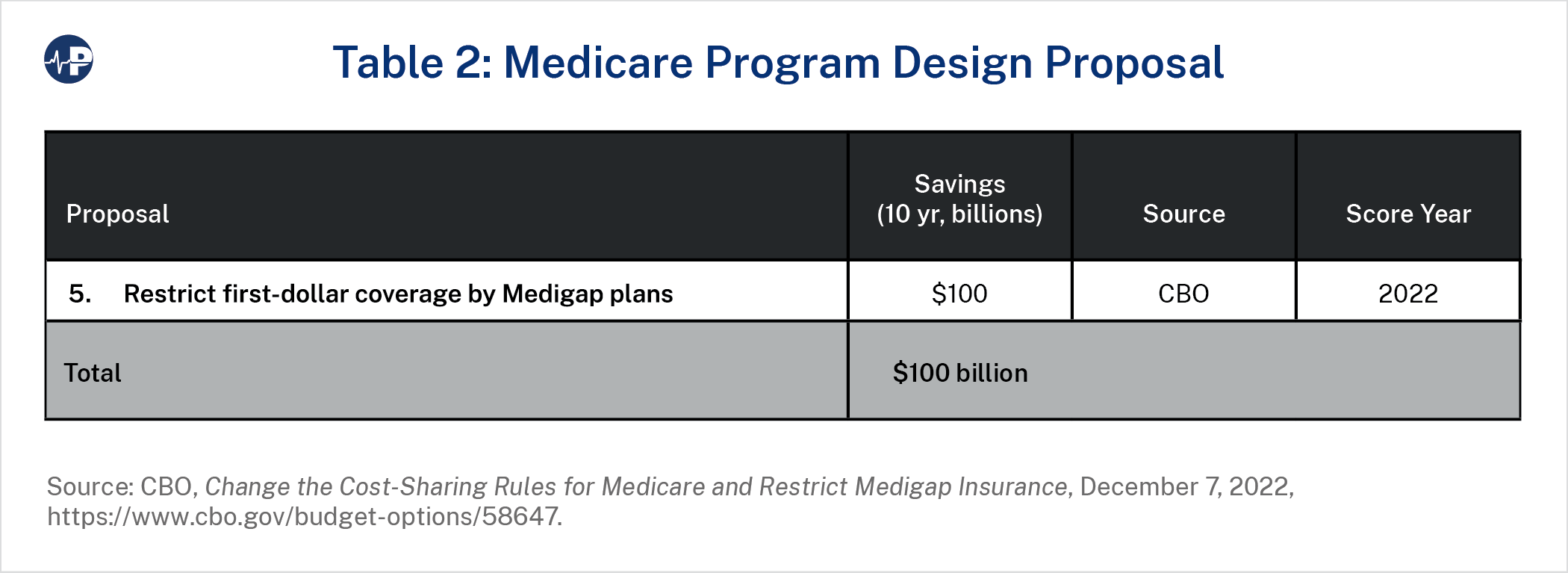
Proposal 5 would restrict Medigap plans from covering cost-sharing up to a certain point and limit additional coverage at 50 percent up to a second threshold, with specific thresholds indexed to FFS spending growth per enrollee. Reforming Medigap plan coverage would make beneficiaries less likely to purchase it, redirecting their spending from Medigap premiums to ordinary FFS cost-sharing. Such changes to Medigap plans could be structured to exempt current beneficiaries or near-retirees in order to minimize disruption, but this proposal would not reduce Medicare benefits or change the program’s eligibility standards. Both parties have supported this proposal in other forms in the past. The Obama administration’s 2016 budget recommended a surcharge for new beneficiaries who purchase certain Medigap plans, while restrictions on Medigap coverage of cost-sharing were also proposed by Senators Joe Lieberman and Tom Coburn and, more recently, by the Republican Study Committee.35
Medicare establishes different payment systems based on the facility where care is delivered. For example, payment for clinic visits in physician offices averages 60 percent less than in hospital outpatient departments (HOPDs).36 The purported justification for this differential is that hospitals tend to have higher expenses and treat sicker patients. However, this gap creates perverse incentives to deliver identical services in costlier settings—leading to more out-of-pocket expenses for seniors as well. Hospitals often acquire independent physician practices and convert them into off-campus HOPDs to obtain higher payments.
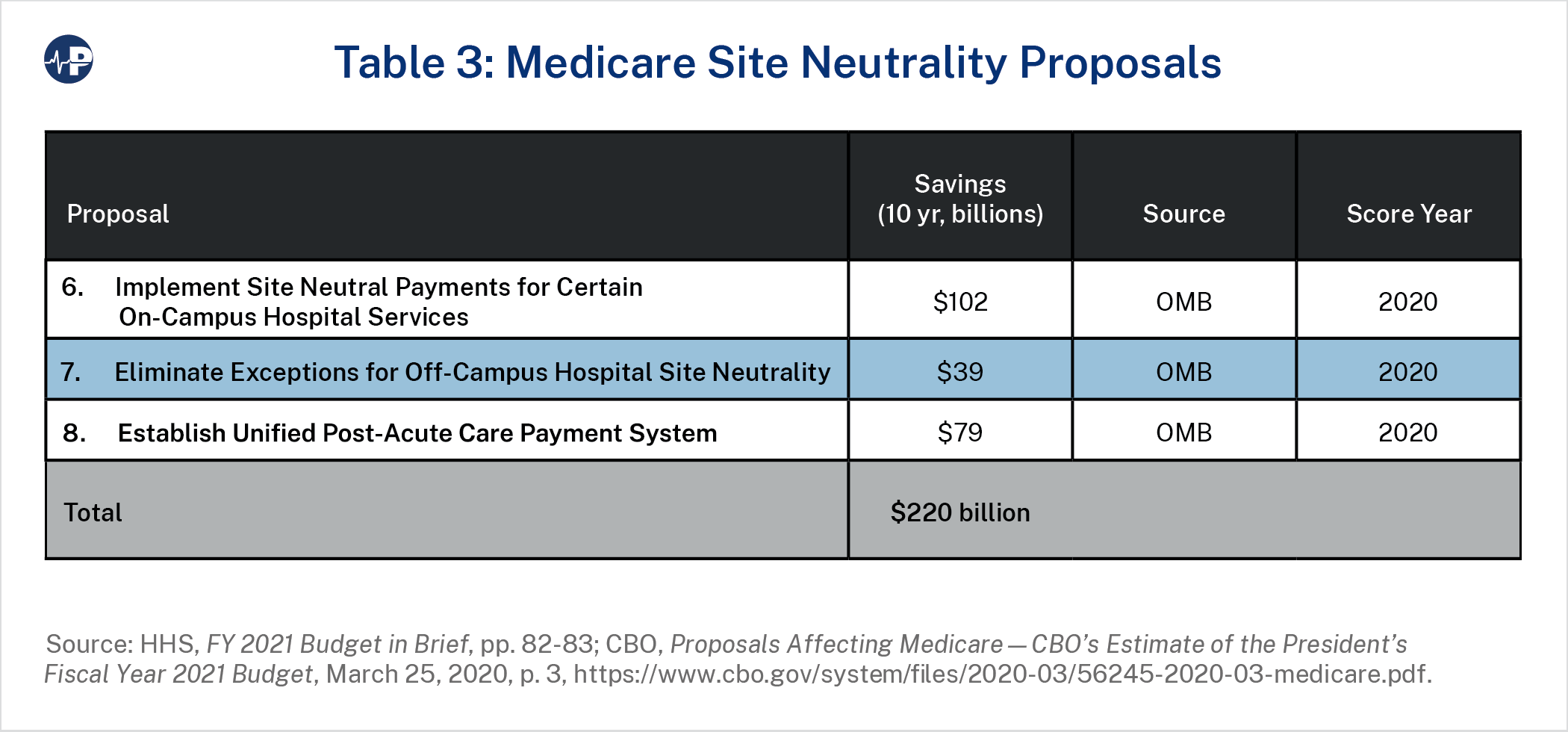
“Site neutral” reimbursement eliminates these incentives by paying the same amount for a procedure regardless of where it is performed. Aligning payment policies can also reduce what seniors pay for these services. Medicare has made some progress in adopting site-neutral payments. In 2018, the Centers for Medicare and Medicaid Services (CMS) finalized a rule to pay for clinic visits in off-campus HOPDs at physician-equivalent rates, as these visits can be performed in physician offices just as well.37 Proposal 6 would apply physician rates to clinic visits and other common services in on-campus HOPDs, which CBO estimated would save about $102 billion.38 Proposal 7 would remove exemptions under the Bipartisan Budget Act of 2015, which requires Medicare to pay off-campus HOPDs at physician rates unless they were operating or under construction before it was enacted. CBO estimated these savings at $39 billion.39
Because Medicare hospital outpatients usually pay 20 percent coinsurance, these reforms would reduce cost-sharing by billions of dollars as well—meaningful savings for many Medicare beneficiaries. The Committee for a Responsible Federal Budget estimated that these hospital reforms (as well as extending site-neutral payments to procedures performed in ambulatory surgical centers) would save the federal government up to $279 billion and save Medicare beneficiaries $137 billion.40
Both the 2016 Obama and 2021 Trump budgets proposed similar reforms to off-campus hospitals.41 Both administrations also supported expanding site neutrality for post-acute care, which Medicare covers following hospital discharge.42 For years, organizations such as the Medicare Payment Advisory Commission presented data suggesting that Medicare overpays post-acute care facilities.43 The IMPACT Act of 2014 required CMS to provide recommendations for consolidating post-acute care reimbursement into a single payment system based on beneficiary health status rather than facility type.44
Proposal 8 slows the rate of post-acute care payment increases over several years before enacting this unified payment system. This would allow the new payment system to set a more appropriate baseline, because establishing a unified payment system in a budget-neutral manner would not address historical overpayments. In aggregate, CBO estimated this would save about $79 billion.45 The Obama administration’s 2017 budget proposed a similar approach by adjusting post-acute care payment updates and bundling payments for postacute care services such that they factor in patient characteristics and lower overall payments.46
These site neutrality proposals would save the federal government $220 billion and reduce patient expenses by simply ensuring that site-of-service decisions are based not on financial incentives but on clinical needs.
Provider Payments
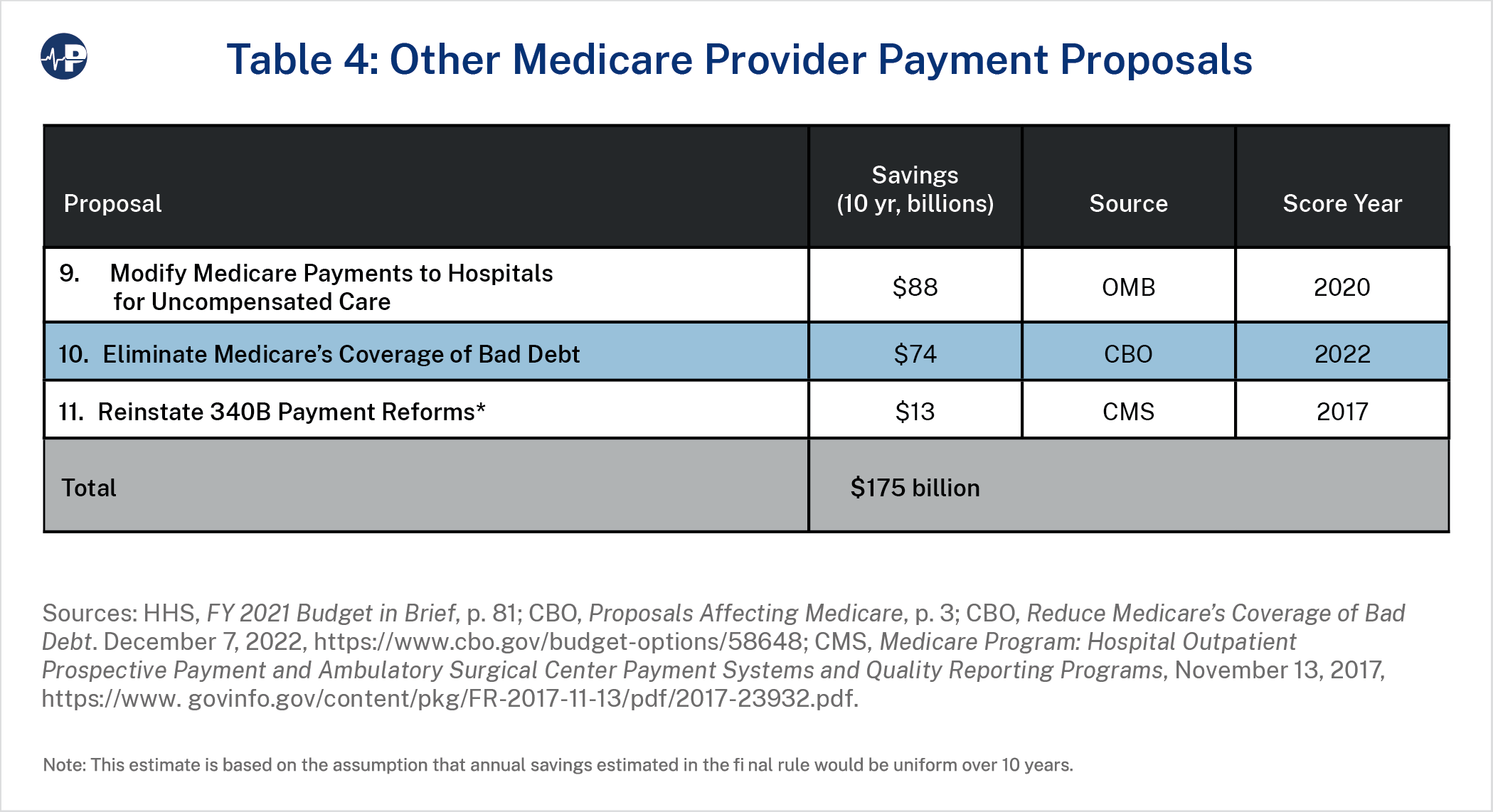
While site neutrality would reduce some excess costs in Medicare, other targeted policies could also have a positive impact. Medicare, unlike private insurers, currently reimburses health care providers for uncompensated care they provide. Uncompensated care consists of “bad debt” (where hospitals anticipate but do not actually collect payment) and financial assistance (i.e., charity care, where hospitals do not anticipate payment). Hospitals that treat a disproportionate share of low-income individuals receive payments based on their share of uncompensated care, which means that Medicare reimburses hospitals for costs that occur outside of the program. These payments do not account for payments these hospitals get from Medicaid.47 Medicare also pays all health care providers 65 percent of bad debt from its beneficiaries, including unpaid costs that state Medicaid programs would usually cover. According to an HHS inspector general’s report, providers sometimes fail to meet federal collection requirements before claiming these bad debt payments.48
Proposal 9 would move uncompensated care funding outside of Medicare, index it to inflation, and distribute it based on hospitals’ share of charity care and non-Medicare bad debt. Proposal 10 eliminates Medicare reimbursement of bad debt. CBO estimates these budget proposals as saving $88 and $74 billion, respectively.49 Proposals to reduce Medicare coverage of bad debt also appeared in the 2017 and 2021 budgets under Presidents Obama and Trump and would reduce providers’ reliance on Medicare subsidies to compensate them for medical debt.50
Proposal 11 would enact reforms to Medicare payment for drugs acquired under the 340B program. Section 340B of the Public Health Service Act allows hospitals to purchase outpatient drugs at a discounted rate (ranging from 25 percent to 50 percent by some estimates),51 but Part B pays for these drugs at the same rate as non-discounted drugs, paying about 58 percent more than the hospitals’ maximum acquisition costs for those drugs.52 Section 340B hospitals are also not required to pass these savings along to consumers. CMS finalized a rule in 2017 reducing Medicare payment for 340B drugs from 106 percent to 77.5 percent of average sales price, which it estimated would save $1.6 billion in total drug payments per year.53
Seniors would directly benefit from lower copays, savings which CMS originally estimated at $320 million annually.54 After litigation under the Trump and Biden administrations, the Supreme Court blocked this rule in 2022, saying that CMS could not target cuts to 340B hospitals without conducting a survey of hospitals’ drug acquisition costs.55
Having Congress enact the 340B reforms in statute would overcome potential legal challenges and save beneficiaries billions over a decade. It would also enable Medicare to retain reduced spending as savings for the program rather than redistribute it elsewhere, as was to occur under the original regulation. Proposals 9 through 11 would result in Medicare savings of $175 billion, plus some out-of-pocket savings for beneficiaries, without cutting benefits.
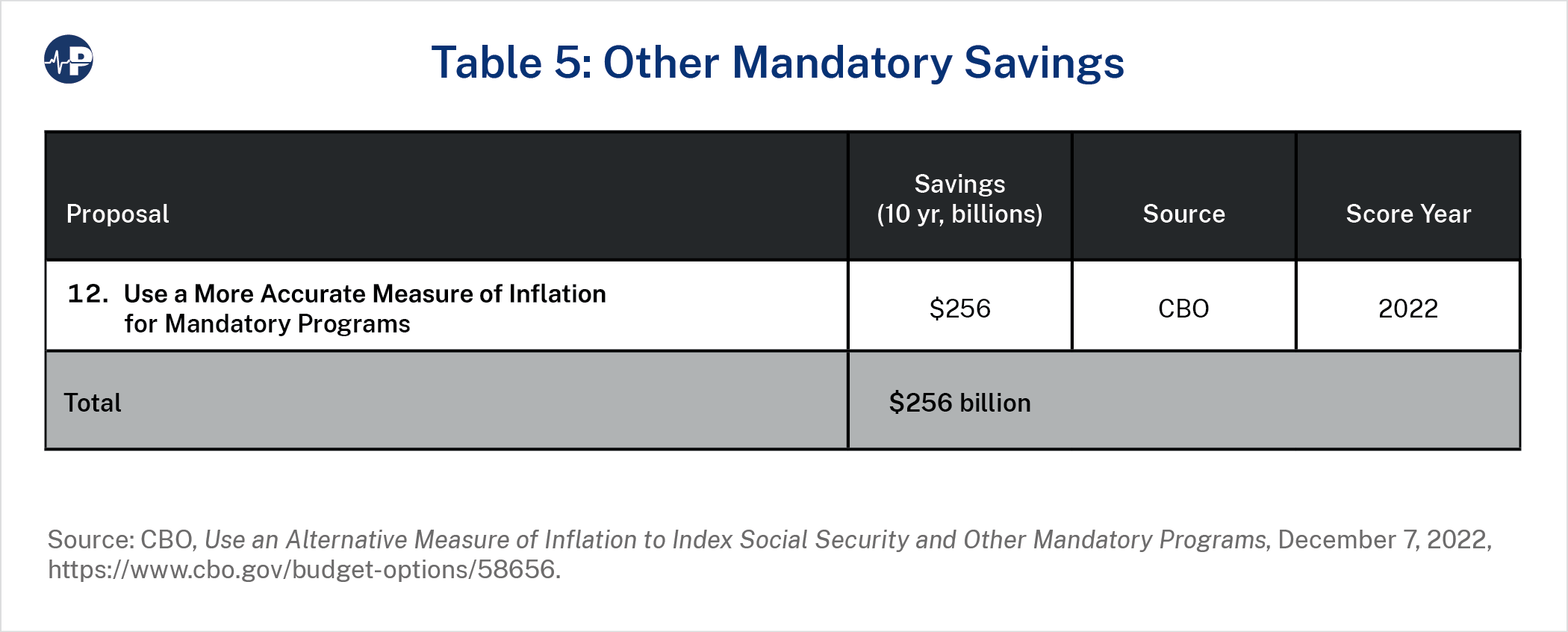
Proposal 12 would impact multiple programs. Mandatory programs (including Social Security) regularly update their spending using a cost-of-living adjustment based on the consumer price index (CPI), which measures the change in price over time for a selection of consumer goods and services. Proposal 12 would instead use chained CPI, which is a more accurate estimate of the actual impact of rising prices because it accounts for the fact that people change their spending patterns—substituting lower-price products for higher-price products—based on relative price changes.56 Chained CPI is currently used for indexing federal individual income tax brackets. Since 2001, chained CPI has grown about 0.25 percentage points slower than traditional CPI on average. The Obama administration’s budget for FY 2014 (released under President Biden’s current chief of staff while he was President Obama’s budget director) endorsed this reform.57 CBO estimates that this policy, which would not change these programs’ benefit structures, would save $256 billion over a decade.58
Additionally, reforming the underlying congressional approach to fiscal policy can increase accountability and contribute to spending reductions. For example, the Statutory Pay-AsYou-Go Act of 2010 (“PAYGO”) already requires that increases in mandatory spending or reductions in federal revenues be offset via sequestration. Congress sometimes suspends these self-imposed rules for major pieces of legislation, lacking the discipline to pay for the cost of their legislation. However, the American Rescue Plan Act (ARPA) did not include such a provision after adding significant new spending, so Congress instead kept these sequester cuts from taking effect through numerous delays.59 OMB estimates that past Congresses have accumulated a PAYGO balance of about $2.4 trillion over the last 10 years.60 Given the current dire fiscal situation, Congress should pay for new spending.
In the 118th Congress, House Republicans replaced PAYGO with a “CUTGO” system in the chamber’s rules, as they did in 2011. This would require new mandatory spending to be offset with equal or greater decreases in mandatory spending elsewhere.61 Adopting such a system across both chambers of Congress would discourage lawmakers from offloading new, open-ending spending programs onto taxpayers. Regardless of the differences between PAYGO and CUTGO, both parties have supported some form of automatic accountability to avoid increasing deficits.62 Congress should actually put those policies into practice.
Congress should also avoid making federal health commitments even more unsustainable. In the past two years, both legislative and executive actions have significantly expanded federal subsidies under the ACA. In 2021, Congress passed ARPA at the urging of the new Biden administration, which increased premium tax credits for plans purchased on ACA health insurance exchanges. Previously, those subsidies were available only to those with incomes between 100 and 400 percent of the federal poverty level, but Congress extended them to higher income households as well. The IRA expanded these temporary provisions to last through 2025. According to CBO, expanding the premium tax credits costs roughly $25 billion per year over the next decade.63
This subsidy largely replaces private spending with government spending, increases aggregate spending (by reducing plan incentives to reduce costs and enrollee incentives to shop for less expensive plans), and benefits those who are in less need of federal support. They also encourage employers to stop offering health benefits, which instead passes along the cost of covering individuals and families onto the federal government. For these reasons, Congress should not extend the enhanced subsidies once they expire after 2025.
It has been 13 years since President Obama remarked that costs in Medicare and Medicaid were threatening the federal budget and needed to be reduced. The need to reform these programs is now more urgent than ever—both to improve the quality of health care services funded by these programs but also to reduce their spending trajectory to avoid massive future tax increases or benefit cuts. Reform is also crucial to ensure that the U.S. government has the ability to respond to future crises, such as wars, recessions, and pandemics. The reforms presented in this paper would collectively save more than what is needed over the next decade to put federal health spending on a sustainable trajectory. Policymakers concerned that rising deficits and debt threaten future American prosperity should seriously consider these proposals.
