
In September 2022 the Office of the Inspector General (OIG) at the Department of Health and Human Services (HHS) issued a scathing report that states are failing to require essential reporting by Medicaid managed care organizations (MCOs)1. Consequently, the Centers for Medicare and Medicaid Services (CMS) does not know how hundreds of billions of Medicaid money is being spent by insurers nor how much value recipients and taxpayers are getting for the massive amount of spending through Medicaid.
Unfortunately, these problems are not surprising. States lack incentives to ensure value from Medicaid. The federal government typically pays about 65 percent of Medicaid’s costs with no cap on federal expenditures. Because of COVID-related Medicaid policies, the federal government now reimburses about 70 percent of program expenditures. Meanwhile, CMS has never prioritized Medicaid program integrity.
Key Takeaways
- Given the failures of insurers, states, and CMS, congressional oversight is desperately needed to ensure recipients and taxpayers are receiving value from Medicaid.
- The ACA and COVID-19 Medicaid policies have exacerbated improper enrollment and spending in the program with now more than 15 million ineligible recipients.
- Medicaid managed care spending now exceeds $420 billion annually, and a new report from the HHS Inspector General shows a lack of accountability with this spending as insurer profits on Medicaid expansion skyrocket.
Medicaid Enrollment and Costs Have Been Surging
The two defining government health policies of the past decade—the implementation of the Affordable Care Act (ACA) and the federal response to COVID-19—have left a legacy of dramatically expanded Medicaid. In June 2022, 82.3 million people were enrolled in Medicaid,2 up from 55.0 million people in June 2013 prior to the ACA expansion of the program.3
The ACA’s expansion of Medicaid to able-bodied, working-age adults caused about half of the enrollment increase. The other half results from increased federal Medicaid funding during the COVID-19 public health emergency so long as states do not make any eligibility changes or remove ineligible recipients. Likely more than 15 million people currently enrolled in Medicaid are not actually eligible.
This enrollment surge is driving a spending flood as well: Medicaid spending increased from $445 billion in 2013 to an estimated $783 billion this year.4
Medicaid Expansion Has Been Very Profitable for Health Insurers
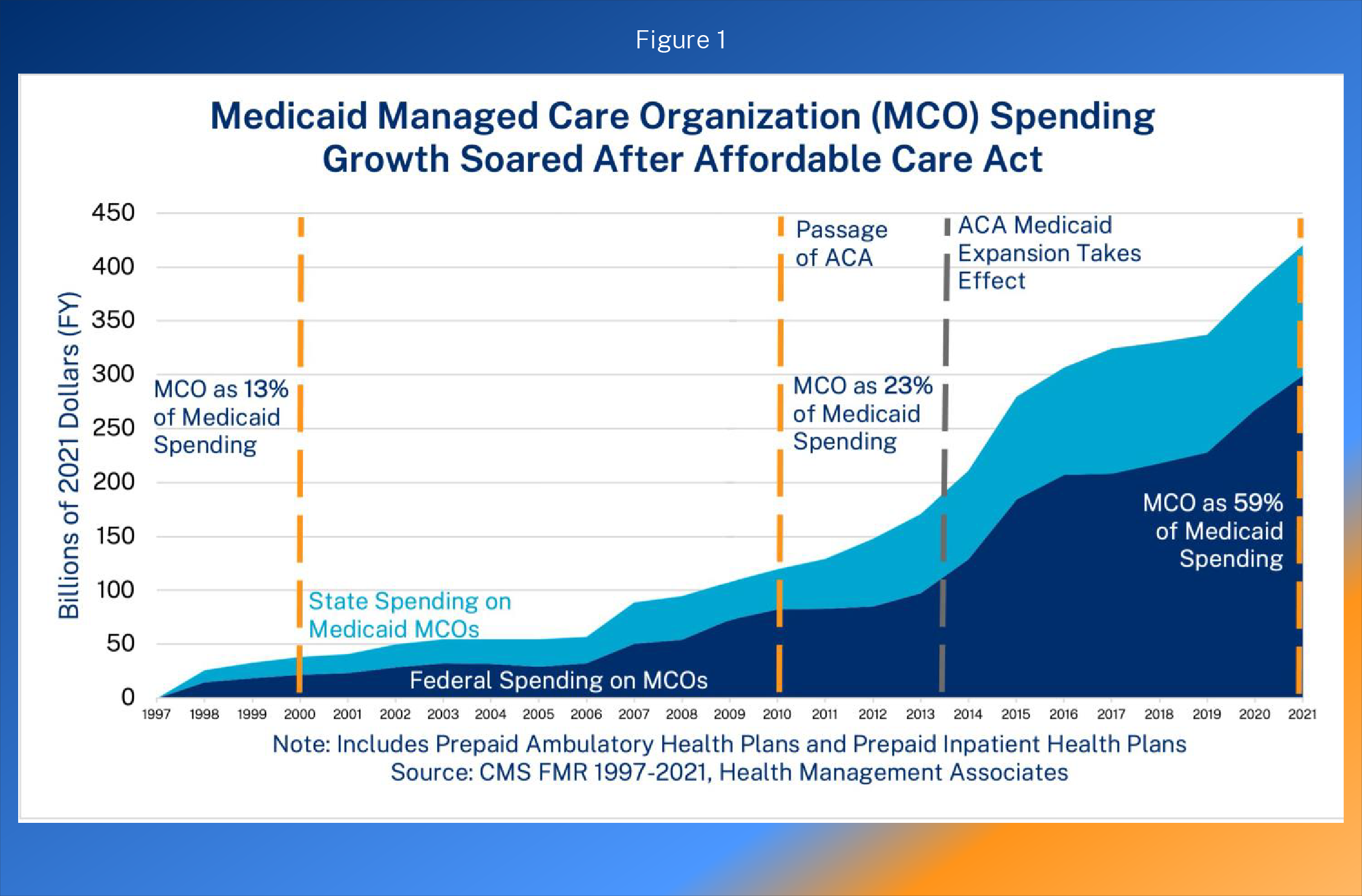
This surge in Medicaid enrollment and spending has drastically increased revenue for insurers participating in Medicaid. Roughly 70% all Medicaid recipients—and a much higher percentage of ACA expansion recipients—are enrolled in managed care.5 Figure 1 shows the growth in Medicaid managed care expenditures. Medicaid spending through managed care has quadrupled after the ACA in inflation-adjusted dollars—up from about $100 billion in 2010 (the year the ACA was enacted) to $420 billion in 2021 (59 percent of program spending).6
The second figure is reproduced from a 2018 White House Council of Economic Advisers report, which showed how health insurer profits soared with the implementation of the ACA, comparing the growth in insurer stock prices with the broader index.
There is a lack of evidence that taxpayers have benefitted or health outcomes have improved from the surge of Medicaid managed care. An empirical economics study found that the growth of managed care in Medicaid through 2009 was associated with somewhat higher spending although there was significant variation across states.7
On health, despite large Medicaid expansion, American life expectancy was lower in 2019 than in 2013.8 From 2013-2017, states that expanded Medicaid actually had worse mortality trends than states that did not adopt the expansion.9
The ACA Has Increased Improper Medicaid Enrollment and Spending
The ACA created a new category of Medicaid recipients—able-bodied, working-age, non-disabled adults. From 2014-2016, the federal government paid all their costs, leaving states without any incentives to ensure that only eligible people were enrolled or that people eligible under previous state criteria (with a much lower federal reimbursement rate) were classified appropriately instead of as expansion enrollees. In addition to the lack of incentive to ensure proper eligibility, states also did not have an incentive to spend judiciously on Medicaid recipients. Thus, states set high payments to Medicaid MCOs on behalf of newly eligible recipients. The ACA also permitted expedited applications, leaving states with fewer eligibility safeguards.10
Medicaid expansion enrollment and spending far exceeded projections. A 2016 study published by the Mercatus Center found that enrollment in expansion states exceeded expectations by about 50 percent and spending per recipient exceeded expectations by about 50 percent.11 Numerous audits by the HHS OIG (summarized in a 2019 Mercatus research study) confirmed that states were careless during this period and failed to properly determine eligibility.12 For example, an OIG review of California Medicaid recipients found that more than half of sampled recipients were ineligible or did not have their eligibility information properly reviewed.13 Some recipients were not even aware that they were enrolled in Medicaid.
Although the federal reimbursement rate for the expansion population has declined to 90 percent, it is still much higher than the rate for traditional Medicaid populations, such as low-income children, pregnant women, and individuals with disabilities—the people for whom Medicaid was intended. This differential in rates means that states still have large incentives to misclassify recipients as eligible under the expansion. The lack of incentives for states to implement program integrity measures benefit the health care industry, including insurers, who persistently lobby for greater subsidies from the government.
COVID-19 Medicaid Policies Have Exacerbated Improper Enrollment and Spending
The Families First Coronavirus Relief Act of March 2020 increased the federal reimbursement of state Medicaid spending by 6.2 percentage points for the remainder of the official public health emergency so long as states did not take steps to remove ineligible recipients or alter eligibility rules. Thus, since early 2020, states have not removed ineligible people from Medicaid. Many Medicaid recipients are no longer eligible—such as people who have taken jobs with workplace coverage, now earn income above eligibility thresholds, have married and have a spouse with employer coverage, have moved out of state, or have died. Of course, many recipients remain enrolled who were ineligible when placed on the program.
The Urban Institute estimated that 15.8 million ineligible people were on Medicaid as of September 30, 202214—a number which will increase as long as the public health emergency is extended. If disenrolled, most of the people inappropriately on Medicaid would transition to another source of coverage, such as employer coverage or a subsidized individual market plan. According to estimates from the Congressional Budget Office, 19 million people are enrolled in multiple sources of coverage.15 The most frequent combination are people with Medicaid and employer coverage.
Where Is All of the Money Going? No One Knows, But Much of It Is Improper
Two reports show that both the federal and state governments have abdicated their responsibilities to ensure that Medicaid spending is lawful and appropriate.
First, a November 2021 CMS report estimated total federal improper Medicaid spending at nearly $100 billion16—or about one quarter of program spending. This estimate is actually too low since CMS halted the eligibility component of audits for one third of states because of COVID.
Second, an HHS OIG report released last month found that states are failing to monitor how insurers are allocating dollars they receive through Medicaid.17 HHS OIG discussed the importance of the medical loss ratio (MLR). The MLR shows the percentage of premiums collected that insurers pay out for health care services plus quality improvements. For Medicaid MCOs, the MLR roughly shows the percentage of government payments that insurers use to pay health care expenses for plan recipients. The MLR for Medicaid MCOs must be at least 85 percent.
From the OIG report:
CMS chose MLRs as a policy tool to apply across the program to ensure appropriate stewardship of Medicaid managed care funds. Federal MLR requirements are intended to ensure that managed care plans spend most of their premium revenue on covered health care services and activities that improve enrollees’ quality of care, thereby limiting the dollars plans can spend on administration and keep as profit.
States’ oversight of their plans’ annual MLR reporting is critical to improve fiscal transparency, monitor costs, and promote high-quality care in Medicaid managed care. States must conduct robust oversight of their plans’ MLR reports to effectively leverage the MLR calculation to ensure appropriate Medicaid managed care spending. …
The report also chronicled the failures of states to ensure proper MLR reporting.
[N]early half of the reports that plans submitted were incomplete, which may present a substantial obstacle to States’ oversight efforts and ability to ensure accurate MLRs. Specifically, the data element for non-claims costs, generally defined as plans’ expenses for administrative services, accounted for the majority of incomplete MLR reports. Missing data on non-claims costs may reduce transparency into managed care spending and limit States’ ability to ensure that plans are appropriately spending Medicaid dollars on the health of enrollees rather than excessive administrative expenses. …
States indicated that they review MLR reports for completeness, but few States identified incomplete reports. In addition, although 26 States reported that they review MLR data elements for accuracy for all of their plans, 16 States responded that they did not review the accuracy of selected MLR data elements for all or some of their plans.
MLR requirements, which essentially cap plan profits as a percentage of expenditures, are generally counterproductive because they incentivize higher spending. But since the nation’s taxpayers need to know how insurers are using the hundreds of billions of dollars in payments they receive from the government—the MLR is useful in Medicaid for oversight, recovery efforts if the government paid too much to the insurer, and assessment of the appropriateness of future rates.
One clear problem is that many states have set very high capitated payment rates to insurers for Medicaid managed care, particularly for the expansion population where the federal government is paying almost the entire cost. In many states, these capitated payment rates were well above insurer expenditures, causing massive profits at companies participating in Medicaid managed care.18 A portion of these excessive profits should be returned to taxpayers, but that cannot happen without proper MLR reporting and related independently audited financial statements.
Another problem noted above is that many Medicaid recipients likely do not know they are enrolled in coverage or have another source of coverage, so Medicaid MCOs are receiving monthly payment rates from the government on behalf of people who are almost certainly not going to incur medical expenses. MLR reporting must accurately account for recipients without any expenditures. Doing so would lead to a decrease in rates.
The HHS OIG report highlights two significant problems. First, nearly half of the MLR reports filed by insurers were incomplete. The most frequent missing element was non-claims costs such as administrative expenses. Second, states did not know that so many reports were incomplete—a testament of the low priority that the government places on the appropriateness of Medicaid payments to insurers even though these payments exceed $400 billion a year. One third of states told the OIG that they do not review the accuracy of the MLR submissions.
Congressional Oversight is Desperately Needed
Medicaid, by far the largest public welfare program, is the fastest growing major government program in the nation. Improper spending is a quarter of total expenditures, and states lack incentives to ensure proper spending since the federal government pays nearly two thirds of program costs. CMS has prioritized maximizing enrollment over ensuring that federal dollars are being effectively allocated and has not even responded to congressional oversight letters from the spring on the high improper payment rate.19
Congress should use its oversight authority to obtain the necessary information to do effective oversight, including using the compulsory process for key documents and communications, depositions, and public hearings. CMS will likely try to delay and obstruct congressional oversight efforts, so Congress should also obtain information from states and federal contractors, including Medicaid MCOs.
Specifically, Congress should obtain information from Medicaid MCOs and state Medicaid agencies that allow them to answer the following questions:
- Which insurers are not submitting complete MLR reports and independently audited Medicaid financial statements to states?
- Which states are failing to independently audit and verify the accuracy and completeness of MLR reports and Medicaid financial statements?
- Have any states done an effective job of reviewing, verifying, and auditing MLR reports and reviewing independently audited Medicaid financial reports? Which states?
- Which insurers (including parent company, subsidiaries, and related parties) contract with the same actuarial services firm (including parent company, subsidiaries, and affiliates) that is also providing Medicaid actuarial services to the state or CMS?
- Which states promptly and publicly post on their websites complete MLR reports, audited Medicaid financial statements, and copies of all the underlying actuarial work and assumptions? Which states refuse to publicly post this information?
- Which states have contract or regulatory provisions requiring Medicaid MCOs with an annual MLR below 85% (or higher percentage set by the state) to return or rebate the difference to the state?
- Have any states recovered money from insurers who were overpaid for Medicaid managed care? Which states? Which insurers? How much?
- Which states have policies and capabilities to sanction insurers for failure to file complete, accurate, and timely Medicaid MLR reports or audited financial statements?
- Which insurers have been sanctioned by state for incomplete, inaccurate, or untimely Medicaid MLR reports or audited financial statements?
- Are any states paying insurers more for ACA Medicaid expansion recipients than actuarially comparable traditional Medicaid recipients?
- Are any insurers paying health care providers higher rates or more favorable terms for the ACA Medicaid expansion population than for traditional Medicaid recipients?
- In addition to Medicaid MCO revenues and profits from Medicaid, what are the estimated revenues and profits of related parties of any kind generated as a result of provider, administrative, reinsurance, or other arrangements with the MCO?
- How many recipients have zero medical claims during the year in which they are enrolled?
- How many enrollees only have medical claims associated with emergency room services?
- How many people insurers have found to be ineligible, for any reason but including through death or move out of state, that they reported to the state government?
- Which insurers receive more than half of their revenue from Medicaid?
Special thanks to Kip Piper for his excellent review and suggestions of oversight options.

